September 2024
Volume 5
Part 7 - Replacement of the gas riser
Part 8 - The London Fire Brigade
HC 19–V
Presented to Parliament pursuant to section 26 of the Inquiries Act 2005
Ordered by the House of Commons to be printed 4 September 2024
This report contains content which some may find distressing.
© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at www.gov.uk/official-documents.
Any enquiries regarding this publication should be sent to us at [email protected].
ISBN 978-1-5286-5080-9
(Volume 5 of 7)
E03165832 09/2024
In his Phase 1 report the Chairman found that the supply of gas to the tower did not play a significant part in the outbreak or development of the fire on 14 June 2017 and that the employees of Cadent Gas Limited who attended to shut off the gas supply made appropriate decisions and executed their task admirably.[1] In this phase of the Inquiry we have investigated the replacement of one of the gas risers between 2016 and 2017. The works had not been finished at the time the fire occurred and we therefore thought it appropriate to consider whether they might have contributed to the spread of smoke or fire within the tower.
On completion of the refurbishment work to the tower in 2016 gas was supplied to residents by two pipelines which entered the basement below ground level on the east side: a ten-inch steel pipe that fed the boilers supplying hot water to residents[2] and a four-inch steel pipe that supplied gas to the flats.[3]
The pipe providing gas to the flats entered the basement at a high level. Four pipes, known as “risers”, ran vertically up into the tower; two of them were then split into two, making six risers in total.[4] These passed through the fabric of the building and directly into a cupboard in each flat. One of the risers supplied gas to all the “Flat 2s”.
The gas supply had been installed at the time the tower was built and by the time of the fire the pipework was almost 50 years old. It did not comply in a number of respects with current regulations.
On 1 October 2016, corrosion of the riser serving the “Flat 2s” made it necessary to cut off the supply of gas to all the “Flat 2s”.
Cadent Gas Limited (“Cadent”) is a gas transporter which owns and operates the pipes and apparatus that transport gas. Cadent does not own the gas itself but is paid by suppliers to deliver it through a network of pipes in a particular area. In the case of Grenfell Tower the area was that served by Cadent’s North London gas distribution network.[5] Cadent was responsible for the safety of the service pipework up to the point of the emergency control valve located at each customer meter; the installation pipework beyond the meter was the responsibility of RBKC as the owner of the building.[6]
The Health and Safety Executive monitors and oversees the health and safety of onshore gas distribution and supply[7] and Ofgem determines the funding and ensures the competitiveness of gas pricing.[8] Since the 1990s, in common with all gas transporters, Cadent is under certain statutory obligations, including obligations to:
Part of Cadent’s strategy to maintain service pipework for buildings in multiple occupation was to conduct a rolling programme of surveys.[12] On 30 September 2016 Cadent carried out a survey on Grenfell Tower[13] and identified three significant problems:
In response to the discovery of the leak Cadent immediately cut and capped the riser which supplied “Flat 2s”. That was completed in the early hours of 1 October 2016.[17]
Cadent used this and other information from the survey to calculate a building priority score[18] which indicated how often a building should be surveyed. The score for Grenfell was such that Grenfell Tower was placed on the list for discussion at the regular Cadent hazard and operability meetings, known as “HAZOP” meetings. The inability to find the missing pipeline isolation valves and the severe corrosion was noted on a schedule presented at the HAZOP meetings of 5 December 2016 and 23 February 2017.[19]
Pipeline isolation valves, by which the supply of gas to a building can be shut off quickly, are the main emergency control mechanism for buildings in multiple occupation.[20] They are mandatory on service pipelines to such buildings[21] and are located outside the premises so that access to them can be obtained easily through valve chambers with marked covers visible at pavement level. For obvious safety reasons, as part of making appropriate arrangements for responding to incidents and emergencies, gas transporters have a duty to maintain access to pipeline isolation valves.[22] Notwithstanding that, we were told that it was well known in the gas industry that pipeline isolation valves are often lost, for example, as a result of being covered over by landscaping or road works.[23] The survey of Grenfell Tower carried out by Cadent in 2008 showed that “fire valves” (another term for pipeline isolation valves) had been installed on the pipes supplying gas to the tower.[24] The fact that Cadent could not find them in 2016 was almost certainly attributable to the landscaping works completed as part of the refurbishment.[25]
Having discovered in October 2016 that the pipeline isolation valves could not be found, Cadent should have taken steps to reinstate them immediately but it appears that the appropriate team in Cadent was not notified about the need for that to be done. Mr Harrison, one of Cadent’s network directors, accepted that that had been a failure on its part which should not have occurred.[26]
The failure to reinstate the pipeline isolation valves did not affect the course of events surrounding the fire because burning debris falling on the east side of the tower would have prevented anyone from obtaining access to them.[27] However, on another occasion access to them might be of critical importance and we therefore think that all gas transporters should have a legal duty to inspect these emergency valves at intervals to ensure that they are accessible and to reinstate them if they are not.
Although steel pipes are very strong and have a long service life under normal conditions, they are susceptible to corrosion, particularly if exposed to damp. Because corrosion causes the steel to deteriorate and lose its integrity, keeping it within acceptable levels is an important part of maintaining the safety of pipelines.
Cadent commissioned a corrosion survey for Grenfell Tower on 5 December 2016.[28] Mr Harrison explained that the survey was not completed because of problems over obtaining access to the tower. A Cadent engineer attended on two occasions but could not get into the relevant parts of the building.[29] Although a decision was made in February 2017 to try again, the full corrosion survey had not been completed by the time of the fire, some eight months after the corrosion had been discovered.[30] As Mr Harrison accepted, that was unacceptable.[31]
After the fire it was found that a riser in Flat 115 had ruptured. It is possible that that was a result of a failure to keep corrosion levels within acceptable limits and occurred during the fire or later as the building continued to deform from its effects,[32] but we do not think it is necessary for us to reach a decision on that question and in any event do not have sufficient evidence to do so with any confidence. All we can say is that several factors may have contributed to the rupture of that particular pipe, one of which may have been corrosion that weakened it at one of its threaded joints.[33]
By June 2017 Cadent’s map of the gas pipes running into the tower should have shown all three systems: the pipe supplying the boilers, the original pipe supplying gas to the flats and the new pipe supplying gas to the “Flat 2s”. However, the maps available to the Cadent engineers who attended the fire only showed the pipe supplying the boiler.[34] Cadent should have known that its maps were inaccurate because those available when it carried out the survey in September 2016 also showed only the pipe supplying the boilers.[35]
Cadent maintained that its failure to correct the maps did not, in fact, have any material effect on the ability of its engineers to identify and isolate the gas supply pipes on the night of the fire, since they were able to obtain the correct information from other sources.[36] That is true, but it was attributable more to luck than good organisation that the engineers concerned happened to know the true layout of the pipework and had accurate information readily available to them[37] as well as the time and the means to provide it to those who needed it.[38]
It is important that all gas transporters have accurate maps of the pipelines serving buildings in multiple occupation.[39] Although Cadent has a process for revising its maps, it was not implemented in good time in the case of Grenfell Tower.[40] Accurate maps are essential in order that operatives can locate the pipeline isolation valves and may be of critical importance in emergencies. There appears to be no good reason why the map was not revised after the 2016 survey, or, failing that, after the installation and commissioning of the new pipe in early 2017.
UK designers of gas supply systems pay particular attention to the standards published by the Institution of Gas Engineers and Managers (IGEM) when planning and executing work of that kind.[41] Although gas engineers should be aware of the Building Regulations,[42] in 2016 there was a strong emphasis and reliance on IGEM publications and there existed within the gas industry a general understanding that if an engineer complied with that guidance, all relevant regulatory standards, including the Building Regulations, would be met.[43] The IGEM publication applicable to the work to be carried out at Grenfell Tower in 2016 was IGEM/G/5, second edition.[44]
Having cut and capped the riser serving the “Flat 2s” on 1 October 2016, Cadent had to consider whether and, if so, how, to reinstate the supply of gas to them.
For that purpose it engaged tRIIO, a consortium formed by Morrison Utility Services Limited and Skanska Construction UK Limited, to design and install replacement gas pipes and connections.[45] tRIIO entered into subcontracts with other organisations and individuals for some of the work.[46] There was plainly some urgency and it is apparent that Cadent sought to reinstate customers’ gas supplies as quickly as possible.[47]
Two options were available to it: it could either find a way to install a new riser to reconnect the “Flat 2s”, or it could pay customers to replace their gas appliances with electric appliances. On 17 November 2016, Cadent rejected the latter option because only part of the building was affected.[48] It therefore decided to restore the supply of gas, provided it could do so safely.[49]
IGEM/G/5 provides a hierarchy of options for siting gas pipes. It states that the best option is an external network of pipes so as to give them direct ventilation to natural air.[50] In the case of Grenfell Tower however, the TMO and tRIIO agreed that installing pipes on the outside of the tower was not practicable because they would pierce the newly installed rainscreen cladding, would compromise the integrity of the facade and potentially invalidate any warranty for the cladding system.[51] In our view, that was a reasonable position for the TMO to take.
tRIIO commissioned Simon Boygle, a surveyor trading under the name of London Ops Gas, to find an alternative route for a replacement riser. He and tRIIO considered several options, including running the new riser in the same place as the original riser, that is, vertically through the floors and ceilings of the flats and directly into the kitchens. That idea was quickly discounted as impracticable, however, because of the difficulties involved in obtaining access to the pipes embedded in the fabric of the building.[52] They also considered running the new pipe through the existing utilities shaft,[53] but that option was rejected, principally because the ventilation was considered to be inadequate.[54]
A key consideration was that any gas pipework must be adequately ventilated so that if a leak occurs it does not cause the atmosphere to become unsafe, with the consequent risk of an explosion. While external ventilation directly to fresh air is preferred,[55] IGEM/G/5 allowed for any steel pipeline that had welded or screwed joints to be ventilated indirectly to outside air through an area that was “normally-occupied”, meaning occupied as an individual dwelling or a common corridor or lobby.[56] However, IGEM/G/5 stated that mechanical ventilation should not be used to achieve the required ventilation level,[57] which in the case of Grenfell Tower prevented siting gas pipes in the lobbies, since they relied on mechanical ventilation. IGEM/G/5 also required ventilation to be provided at the top and bottom of every fire compartment,[58] consistently with the guidance in Approved Document B relating to ventilation in protected shafts.[59] Approved Document B also provided further guidance on the ventilation of shafts, directing the reader to BS 8313:1997 on the size of ventilation openings.[60]
It is clear that there were two requirements that had to be taken into account: ventilation for gas safety and compartmentation for fire safety. Giving appropriate recognition to each of them is a challenge for anyone seeking to supply gas to any complex building in multiple occupation.
On 12 October 2016 Simon Boygle proposed that a new riser should be installed in the stairwell of Grenfell Tower.[61] That was the only means by which to satisfy the twin requirements of ventilation and compartmentation.[62] The new riser would travel from the basement, through the lower floors, through the stairs, and then by means of laterals restore the supply of gas to the “Flat 2s”. It was envisaged that at a later date the pipework would be extended to serve all the flats in the tower and the original pipework would be decommissioned.
What nobody involved in the project understood at the time was that although both IGEM/G/5 and Approved Document B allowed gas risers to be placed in protected stairs,[63] if the stairs were also firefighting stairs, additional protections were required.[64] Diagram 52 in Approved Document B advised that firefighting stairs should be constructed in accordance with BS 5588-5:2004,[65] which in turn advised that such a shaft should contain only services associated with fire-fighting. In other words, the guidance in Approved Document B and the British Standard to which it referred was that gas supply equipment should not pass through the same compartment as services associated with firefighting.[66] Although it is arguable that appropriate standards of safety could have been achieved by separating the riser from the firefighting stairs with fire-resisting construction, as was explicitly permitted for gas pipework in protected stairs,[67] the position is not clear in the guidance document or standards in relation specifically to firefighting stairs. We note that the first design did not have any boxing protecting the riser in the stairs.
That special consideration had to be given to firefighting stairs does not appear to have been widely understood in the gas industry before the Grenfell Tower fire[68] and there is no evidence that any other professional expressly considered the point.[69]
tRIIO’s first design did not provide much detail of how the ventilation of the pipework would be achieved.[70] The riser was to be constructed of steel with welded joints, so indirect ventilation was available as a design choice pursuant to the guidance in IGEM/G/5.[71] On that basis the design included the following features:
No analysis was made of the ventilation available for each space through which the gas pipes were to pass.[77] In our view, such a complicated design required detailed consideration of the ventilation arrangements in order to demonstrate that the pipework would be ventilated adequately and safely.[78] tRIIO did not carry out a detailed analysis of that kind.
A detailed risk assessment should also have been carried out.[79] According to IGEM/G/5, designers of gas pipework in buildings in multiple occupation should carry out a risk assessment to identify and mitigate hazards and maintain a written record of the results.[80] In late 2016 tRIIO’s procedure was to record risks in its CDM Design Risk Register, which took the form of a spreadsheet that generated an initial risk score. If that score was 18 or more, tRIIO would carry out a fuller assessment by responding to a list of more probing questions.[81] tRIIO completed the CDM Design Risk Register in relation to Grenfell Tower on 15 November 2016. It generated a score of 17.[82] Although the designers could have manually over-ridden the process and carried out a fuller assessment of risk, they did not do so.[83]
We do not think that tRIIO’s risk assessment process was adequate for buildings in multiple occupation.[84] We note that tRIIO’s own CDM Design Risk Register shows that any building of that kind would be “high risk” in and of itself[85] and accordingly, the process should have required that it be the subject of a fuller assessment. That was particularly so in the case of an old building such as Grenfell Tower in circumstances where the proposed design was relatively complicated. tRIIO should therefore have overridden the scoring system and considered the risks posed by the installation in more detail. Mr Dolan, tRIIO’s director of operations, accepted that it had been at fault in failing to do so.[86]
Cadent’s contract with tRIIO did not require it to check design decisions and it did not expect to do so. However, once work began, Cadent was under a statutory duty to notify the Health and Safety Executive (HSE) using the form “F10”.[87] tRIIO had produced an F10 covering all the work it intended to carry out during the period 2016-2017,[88] but that did not constitute an adequate notification of the work at Grenfell Tower. Cadent should have produced an F10 to notify the HSE of that work.[89] A generic F10 of the kind produced by tRIIO was inappropriate for a project affecting a large building in multiple occupation.[90]
Over the course of some months the original riser was replaced using a new pipe which entered the basement below ground level on the east side.[91] From there it passed up through the lower floors and into the stairwell where it passed through holes cut in the floors of the landings.[92] If the supply of gas was to be restored to a flat, a horizontal pipe, or ‘lateral’ was led from the riser through the stairwell wall and into the lobby.[93] The lateral then passed round the perimeter of the lobby just below the ceiling and a pipe from it entered the relevant flat through a hole in the wall between the flat and the lobby.[94] The pipe was connected to a meter which had to be moved from its original position in the kitchen to the hallway near the front door.[95] Further pipework was then installed between the meter and any kitchen appliances that burned gas.
After the gas pipework had been installed into the tower it was commissioned on 10 March 2017,[96] even though the work in the lobbies of boxing it in had not been completed. At that stage the work did not comply with the guidance in IGEM/G/5 because a leak in the lobby would have been ventilated by mechanical ventilation, which was not permitted. It appears that tRIIO took a calculated risk and reconnected the supply of gas to customers before all the work had been completed. We understand the desire to reconnect occupants as quickly as possible, but the fact remains that tRIIO should not have introduced gas into a pipeline without all the ventilation requirements being in place.[97]
On 21 March 2017, tRIIO’s design manager inspected the work and noted that flanged joints had been installed rather than welded joints.[98] Flanged joints have a compression fitting which seals the connection between the two pipes with a gasket, as opposed to screwing or welding the pipes together.[99] As a result, flanged joints are more prone to leaking and could not be used if the stairwell was to provide the necessary ventilation.[100] The installation of the flanged joints compromised the ventilation strategy and the error was not noticed by tRIIO’s design team before gas was reintroduced into the pipeline.[101]
On 24 March 2017, in response to that discovery, tRIIO introduced a modification to the arrangement, under which the vertical riser (as well as the laterals) was to be fully boxed-in, both in the stairwell and also throughout the lower levels and the basement, using materials with a two-hour fire rating.[102] Intumescent vents were to be installed in the boxing in the stairwell, which would close in the event of a fire but allow for some ventilation in normal circumstances.[103]
The description of the modified arrangement did not show how the boxing-in was to be achieved at the lower levels, i.e. through the utility duct and in the storeroom and basement. Nor did it show how the boxing-in would be connected to the vent in the roof.[104] Moreover, the new design created other problems in relation to ventilation. It assumed that air would circulate within the boxing and across the pipework through the holes in the landings and the walls between the stairwell and the lobbies, but the holes through the landings had not been enlarged to allow for a flow of air within the new boxing.[105] There was no evidence that calculations had been carried out to determine the size of the holes that would be required nor was it clear how an increase in the size of the holes and the boxing could be accommodated given the narrowness of the stairs.[106] The use of intumescent vents was not consistent with the requirements of IGEM/G/5.[107]
In this case tRIIO manually over-rode its CDM Design Risk Register process and carried out a full design risk assessment that was recorded on a four-page spreadsheet identifying factors for consideration.[108] Three of those factors related specifically to buildings in multiple occupation, namely, breach of compartmentation, failure due to thermal expansion of south-facing pipes, and ventilation.[109] They were appropriate matters but they did not cover everything that a designer ought to consider, such as, for example, means of escape in fire, corrosion, inspection and maintenance, and valve access and security.[110]
In addition, the information tRIIO added to the Design Risk Register lacked sufficient detail. On the important question about fire compartmentation, the action recorded was simply to follow the Building Regulations and Fire Safety Order and seal the compartments accordingly. A gas engineer was to review the arrangements for ventilation, although they were not described in any detail in the design. Mr Dolan accepted that the assessment process fell below the standard required and that a more detailed consideration of matters affecting buildings in multiple occupation was needed.[111]
Although tRIIO adopted a more formal approach to the modified arrangement, there is no evidence that anyone calculated the amount of ventilation needed for the pipework.[112] That was particularly important, given that the ventilation strategy had changed and that the degree of ventilation had been reduced by the boxing-in of the entire pipeline.
Regrettably, tRIIO and its sub-contractors continued to make mistakes during the construction of the work. As Mr Dolan and tRIIO accepted,[113] although the boxing-in of the pipework should have been carried out using two-hour fire-rated materials[114] (and although the TMO was told that it would be),[115] the sub-contractors, Express Building Contractors Ltd, in fact used materials that were rated as having a fire integrity of only 88 minutes.[116]
A further problem also arose from the need to move the gas meters from the kitchens closer to the front doors because tRIIO’s specifications required that there be no more than two metres of service pipework inside a residential property.[117] As a result, a sub-contractor of K&S Pipe Contractors, Holland Gas Engineers Ltd, was obliged to place meters in or adjacent to the entrance hall, which was the only escape route.[118] Meter points can present a particular fire risk because if there is a fire, gas can burn freely from open meter ends. IGEM/G/5 suggests relatively easy mitigations, including installing the meter inside a 30-minute fire-rated cupboard with a self-closer or installing a thermal cut off device[119] to stop the flow of gas either before or after the emergency control valve.[120] However, neither of those steps were considered at Grenfell Tower.[121]
tRIIO maintained that the meters were often sited in an alcove or cupboard adjacent to the entrance hall and that the mitigation measures mentioned above were unnecessary.[122] However, we have seen examples of meters being located behind curtains[123] or behind doors that had rising hinges and were not self-closing[124] and it is plain that in some cases the meter was sited close to the escape route from the flat. Although there is no evidence that any of the meters played a role on the night of the fire, we do not consider those arrangements to have been satisfactory.
There is no evidence that gas leaked from any part of the new installation during the fire on 14 June 2017.[125] However, the works had not been completed by that time. The boxing-in in the stairs had almost been completed, with only the top floor and the connection to the roof vent outstanding, but the boxing-in of the laterals in the lobbies had not been completed, except on floor 5. Battens had been installed for the boxing-in in the lobbies on floors 4, 8, 9, 10 and 11 only. Mr Dolan estimated that the remaining work would have taken about five weeks.[126]
While the work was being carried out the oversized holes between the stairwell and the lobbies were not temporarily fire-stopped. It was possible, therefore, for smoke to move from one compartment space to another. Heavy smoke staining on the internal faces of the boxing in the stairs indicates that some smoke must have travelled from the lobbies into that boxing.[127] There was also evidence of staining between adjacent floors which appears to indicate that smoke had travelled between floors through the boxing of the riser.[128] It is possible, therefore, that during the fire smoke may have travelled from one lobby into the boxed-in riser and out into lobbies on other floors higher up the tower, thereby compromising the compartmentation between the lobbies. It is not possible, however, to know how much smoke may have travelled in that way or at what stage in the fire. We think it is likely to have been a much less significant route of smoke spread than open fire doors between the lobbies and the stairs.
In March 2017 Cadent expressed concern to tRIIO about the oversized holes between the lobby and the stairwell, which it thought might create an unsafe situation in the event of a fire.[129] In those circumstances we think that tRIIO should have made sure that those holes were temporarily fire-stopped while the work remained incomplete,[130] as Mr Dolan accepted.[131] We are unable to tell whether the failure to do so had any adverse consequences on the night of the fire, but we think it important to record that the risks should have been identified and mitigated during the work.
One question we thought it appropriate to consider is whether the work involved in the replacement of the gas riser required building control approval. In 2016, the gas industry did not routinely consult building control in relation to reinstatement work.[132] In this instance, although Carl Stokes advised that the work was notifiable,[133] tRIIO did not consult building control because it thought that the work did not require approval, despite the material changes to compartmentation that the riser design entailed.[134] In March 2017 Janice Wray told John Allen, the head of RBKC’s building control department, that the new riser had been installed in the staircase and invited him to send a team to the site to look at the work.[135] However, he told her that the riser works were regarded as a repair and were a matter for a fire risk assessment.[136] tRIIO, for its part, appeared to believe that, if carried out in accordance with IGEM/G/5, the work would comply with the Building Regulations but that the TMO would make any necessary application for building control approval.[137]
Whether the work of replacing the gas riser required building control approval is a difficult question on which the evidence does not enable us to express a clear conclusion. However, we think that in cases where the structure of a building on which effective compartmentation depends is affected by the replacement of existing services, careful consideration should be given to the need to obtain building control approval as well as complying with any relevant industry guidance.
In chapter 7 of his Phase 1 report the chairman described the statutory responsibilities, structure and organisation of the London Fire Brigade (LFB). In particular, he described in some detail the operation and management of the control room, the systems and procedures employed in it and the method of handling emergency calls. Later in the same chapter he described operations at the incident ground, with particular emphasis on the role and responsibility of the incident commander and support available from monitoring officers and command units. It is not necessary for us to repeat any of that in this report.
In that report the chairman expressed the view that there had been significant shortcomings in the way the LFB had responded to the fire at Grenfell Tower, both in the control room and on the incident ground, many of which were the result of a failure to provide its control room officers and firefighters at all levels with the skills, preparation and training needed to enable them to respond effectively to the situation they faced. He therefore considered it necessary in this second phase of the Inquiry to examine the organisation and training of the LFB in the years preceding the fire with a view to understanding how that situation had come about and how it might be avoided in the future.
We begin this Part of our report with a brief description of the way in which the management of the LFB is organised to enable the reader to understand the complicated structure that existed in the years immediately before the Grenfell Tower fire. That structure is of importance only because it sheds light on the way in which the organisation functioned during that period. We follow that with a description of the way in which training was organised and training packages obtained from the LFB’s provider, Babcock. It was essential to train officers at all levels in order to meet the challenges of incident command and to ensure that operations were conducted effectively. In view of the criticisms of the LFB made by the chairman in his Phase 1 report we considered it appropriate to pay particular attention to that aspect of the brigade’s management, particularly since it had been the subject of a specific recommendation by the coroner who conducted the inquests following the Lakanal House fire.
Although the fire at Lakanal House in 2009 emphasised the dangers posed by the use, especially in high-rise buildings, of certain kinds of materials and methods of construction, the sources of that knowledge had been available for some years. We therefore decided that we should investigate the extent to which the LFB had been aware of those dangers and, if so, how widely the information had been shared within the organisation. We have also considered other sources of information that were available to it in order to understand why the dangers of a loss of compartmentation and the rapid spread of fire were not understood or recognised by operational station crews.
One important aspect of preparation is gathering information about buildings that may present particular challenges. The LFB is unusual in having a large number of high-rise buildings in the area for which it is responsible, many of which pose particular challenges. We have therefore examined and report on the steps taken by the LFB to collect information about buildings, particularly those that may present particular challenges in the event of a fire.
The response of the control room to the huge volume of information it received as a result of the fire made it necessary for us to examine the quality of the training delivered to control room staff during the years leading up to it. That in turn required us to examine the way in which the control room had been managed and the importance attached to the delivery of regular training, particularly in handling calls from or about people trapped in high-rise buildings. In this Part, therefore, we set out our findings on those matters.
There are other aspects of the response to the fire that in our view called for examination. One significant obstacle encountered by the firefighters who entered the tower was the difficulty of maintaining effective radio communication. We have therefore considered the nature of the equipment then in use, the source of the difficulties in maintaining communication with the bridgehead and the steps that might be taken to overcome them in future.
Maintaining an adequate supply of water also presented difficulties. We have therefore examined the means by which water is made available for firefighting and the steps that were taken by the water undertaker, Thames Water, to improve the supply while the fire was being fought. We have also considered the equipment available to firefighters to deliver water at the fireground and the way in which it was used during the course of the fire.
This chapter provides a broad overview of the organisational structure of the LFB in the period leading up to June 2017. It is necessary to be aware of the key elements of that structure in order to understand which departments and individuals were responsible for different aspects of its functions before and at the time of the Grenfell Tower fire.
On 1 October 2007, Ron Dobson was appointed LFB Commissioner, a position which he held until his retirement on 31 December 2016.[138] Following a period of handover from September to December 2016, Dany Cotton was appointed interim Commissioner on 1 January 2017 and subsequently appointed to the substantive rank on 14 June 2017.[139] The permanent appointment on 14 June had been planned and was unrelated to the Grenfell Tower fire.[140]
The London Fire and Emergency Planning Authority (LFEPA) was abolished on 1 April 2018 and replaced by the London Fire Commissioner, who became the fire and rescue authority for Greater London. The London Fire Commissioner assumed responsibility for LFEPA’s statutory obligations under the Fire and Rescue Services Act 2004 outlined above.[141] On 31 December 2019, Ms Cotton retired as Commissioner and was succeeded by Andrew Roe on 1 January 2020.
As an organisation the LFB was divided into three directorates, the heads of which reported directly to the Commissioner and were responsible for a number of different departments. The internal structure of the directorates was complex and subject to frequent changes, most notably in 2015 following a wide-ranging reorganisation of the LFB as a whole. In the following paragraphs we give a broad and simplified description of the LFB’s structure before and after 2015, focusing on the departments and functions which are most relevant to the Inquiry’s investigations.
Before 2015, the LFB’s three directorates were the Deputy Commissioner’s directorate, the Directorate of Operational Resilience and Training (together sometimes known as the two operational directorates) and the Directorate of Financial and Contractual Services.
Rita Dexter served as Deputy Commissioner between November 2009 and March 2015.[142] In addition to deputising for the Commissioner, the Deputy Commissioner was responsible for the following departments within her directorate: Operational Prevention and Response, Fire Safety Regulation, Strategy and Performance, Communications, and Legal and Democratic Services.[143] The first three of those departments are relevant to the Inquiry’s work.
The Operational Prevention and Response department[144] was responsible for the planning, direction and delivery of the LFB’s operational service, mobilising crews and community safety,[145] including overall responsibility for the control room, fire stations and the collection, management and use of operational risk information.[146] At all relevant times, the LFB’s 102 fire stations were grouped by the 33 London boroughs in which they were located,[147] each headed by a Borough Commander. The boroughs were in turn grouped into four Areas (North East, North West, South East and South West) each headed by an Area Deputy Assistant Commissioner (DAC). Before 2012, many of the department’s responsibilities were split geographically between North London and South London, each headed by an Assistant Commissioner (AC). However, from June 2012 the role and responsibilities for the whole of London were brought together under a single Head of Operational Prevention and Response.
The Fire Safety Regulation department had two broad functions: Regulatory Fire Safety and Community Safety. The Regulatory Fire Safety arm of the department was headed by two DACs, who filled the roles of Head of Fire Safety Delivery and Head of Fire Engineering and Specialist Fire Safety.[148]
Fire Safety Delivery included the department’s fire safety teams, which had responsibility for managing the LFB’s audit and enforcement activities under the Regulatory Reform (Fire Safety) Order 2005 (the Fire Safety Order). As with the Operational Prevention and Response department, the Fire Safety Delivery arm of the department was split into the same four geographical London areas, each headed by an Area Fire Safety Manager, and further divided by boroughs.[149] Fire Safety Delivery was responsible for the LFB’s programme of fire safety audits carried out by fire safety inspecting officers, who could be from either operational or non-operational backgrounds.[150] Some fire safety inspecting officers received additional training to enable them to act as fire engineering liaison officers, who provided support to the more specialist fire engineering teams in relation to building control consultations.[151] Fire Safety Delivery included the Fire Safety Enforcement team, headed by Andrew Jack, which was responsible for reviewing enforcement notices produced by inspecting officers, interpreting legislation and overseeing enforcement prosecutions.[152]
Some senior operational officers were also senior fire safety officers. Senior fire safety officers were typically station managers or group managers who were not part of the Fire Safety department but who would be mobilised to attend incidents requiring four or more pumps to provide support to the incident commander.[153] They undertook a relatively broad, short training course in the basic principles and practice of fire safety to enable them to fulfil that role.[154] In practice, and as happened at Grenfell Tower,[155] it was common for officers who were mobilised to incidents as senior fire safety officers to be assigned different roles by incident commanders.[156] AC Daly, sometime Head of Fire Safety, said that, in his view, this practice of re-assigning senior fire safety officers to operational roles reflected a failure to give priority to fire safety expertise on the incident ground.[157]
The Fire Engineering and Specialist Fire Safety arm of the department included its more technical fire safety teams, such as the Fire Investigation and Fire Engineering teams. Fire Engineering, also known as the Fire Engineering Group, comprised a team of around 10 specialist fire engineers who held, or were studying for, degree-level qualifications in fire engineering.[158] Led by two Senior Fire Engineers, the group’s main function was to consider complex references from building control bodies that were beyond the experience of inspecting officers.[159] Most of the group’s work consisted of providing support to external bodies, though the group also contributed to the development of LFB policy as part of the standard process of internal consultation.[160] Fire Engineers were not involved in the development of operational training unless they were specifically asked to contribute their expertise.[161]
The Fire Investigation team was made up of watch-based operational personnel whose function was to attend incidents to investigate the cause of the fire. The team used the information collected from such inspections to identify trends with a view to informing activities within the LFB and to advance the work carried out by the LFB with external bodies, including those in industry, to improve fire safety across the built environment.[162]
The other arm of the Fire Safety department, Community Safety, concentrated on actions designed to prevent fires (such as home safety visits), on people at particular risk and on community behaviour.[163]
The Strategy and Performance department led the LFB’s work relating to the integrated risk management plan (the London Safety Plan), its internal risk management planning, and performance reviews.[164] Despite its name, the department was not in fact central to the strategy or performance of the LFB’s core operational responsibilities.
AC Gary Reason was appointed Director of Operational Resilience and Training in January 2012.[165] On his retirement in January 2015, he was succeeded by AC James Dalgleish.
The Directorate of Operational Resilience and Training comprised the following departments: Operational Procedures, Operational Assurance, Operational Resilience, and Human Resources and Development.
The Operational Procedures department was responsible for the creation and maintenance of the vast majority of the LFB’s operational policies,[166] subject to certain exceptions, such as the Incident Command policy, for which Operational Assurance was responsible.
The Operational Assurance department was primarily concerned with ensuring effective incident command, the safety of operations and the management of risks on the incident ground.[167] Dany Cotton, who headed the department from its inception in 2012 before her term as Commissioner, said that it was designed to provide combined and streamlined leadership of two existing LFB functions, the Operational Review team’s quality assurance of incident ground operations, and the Health and Safety team’s learning from incidents to identify risks to LFB staff.[168] The department was responsible for producing six-monthly reports which identified risks and trends from an analysis of a wide range of sources, including the LFB’s Incident Monitoring Process Database (IMPD), significant incidents, incident accident reports, fire investigation reports, training and sources from outside the LFB.[169] The department was also responsible for overseeing the production of articles for Operational News, the LFB’s internal circular, by which it sought to draw the attention of staff to some of the risks it had identified and any lessons to be learnt.[170] The functions of the Operational Assurance department were such that it was ultimately responsible for ensuring the operational effectiveness of the LFB and for ensuring that LFB staff were aware of, and adequately prepared to deal with, operational risks which might affect their safety.
Key teams within the Operational Assurance department included the Incident Management Policy Group (also known as the Incident Command Policy Group), which was responsible for collating the information from the sources mentioned above and producing the six-monthly reports for the Operational Directorates Co-ordination Board (the co-ordination board),[171] and the Operations Review Team, which provided oversight of the LFB’s operational activities and routine training designed to maintain and develop operational skills.[172]
The Operational Resilience department included contingency planning and a special operations group focused on policies, procedures and the provision of equipment related to terrorism.
The Human Resources and Development department, previously the Training department, was responsible for the management of the LFB’s contract with its external operational training provider, Babcock Training Limited (Babcock), as well as the LFB’s human resources function.[173] The LFB’s operational training structure and the adequacy of particular aspects of the operational training that existed at the time of the Grenfell Tower fire, is covered in more detail below. The training of control room staff, which was not included in the Babcock contract, is covered separately in Chapter 78.
The Directorate of Finance and Contractual Services, led by Sue Budden, carried out the LFB’s non-operational functions, including Financial Services, Information and Computer Technology and Procurement. It is, on the whole, not relevant to the work of the Inquiry.
Before 2015, the title of Third Officer was held by a senior operational officer in addition to their day-to-day responsibilities. Its purpose was to ensure that there were three senior uniformed officers (the Commissioner, the Director of Operational Resilience and Training, and the Third Officer) able to provide operational cover for serious incidents. From 2010, the position of Third Officer was held by David Brown, who was then an Assistant Commissioner.[174]
In 2015, the LFB underwent an internal reorganisation and the rank of Deputy Commissioner was dropped. Commissioner Dobson said that the position was no longer required as the directors were able to deputise for him within their own areas of responsibility. In broad terms, the Deputy Commissioner’s directorate was reorganised into a new Directorate of Operations. The former Directorate of Operations, Resilience and Training was renamed the Directorate of Safety and Assurance, and the Directorate of Finance and Contractual Services continued as before. In addition to some internal restructuring within each directorate, some departments and functions were moved between directorates.
The separate role and title of Third Officer also ended, as there were now three senior uniformed officer positions: the Commissioner, the Director of Operations and the Director of Safety and Assurance.
The newly created Directorate of Operations retained responsibility for many of the departments which had previously reported to the Deputy Commissioner.
The Fire Safety Regulation department, now simply called “Fire Safety”, continued to incorporate the LFB’s fire safety (including Fire Safety Enforcement and Fire Investigation), fire engineering and community safety functions.
The operational firefighting and control functions of the previous Operations, Prevention and Response department were divided between two new departments: Fire Stations and Central Operations and Control and Resource Management.[175]
AC Brown was appointed Director of Operations in April 2015. When he retired on 31 March 2017, he was succeeded by DAC Philip Thomas George (known as Tom George).[176]
The newly renamed Directorate of Safety and Assurance continued to include Operational Procedures (re-named Operational Policy), Operational Assurance, and Operational Resilience. The Human Resources and Development department was renamed Development and Training, with its human resources functions moved to the Legal and Democratic Services department within the Directorate of Finance and Contractual Services. Health and Safety and the Operational Review Team, previously sub-departments of Operational Assurance, now reported directly to the Director.
Following the restructuring, on 1 December 2015 AC James Dalgleish assumed the position of Director of Safety and Assurance on an interim basis before Dany Cotton’s appointment as Commissioner.[177] Upon Ms Cotton’s appointment, AC Stephen Apter became Director of Safety and Assurance in December 2016. He was in post on 14 June 2017.[178]
This section describes the principal LFB boards and committees which existed before and after the 2015 restructuring.
The Corporate Management Board was the LFB’s highest-level committee, with a membership comprising the Commissioner, the three directors and some heads of department, with other officers and advisers attending when required. The Corporate Management Board held regular meetings and provided a forum for the LFB’s most senior officers to discuss operational, managerial and strategic matters. It also reviewed key papers and reports before they were submitted to the LFEPA Strategy Committee for oversight.[179]
There was also a smaller, informal leadership group known as “the Commissioner’s Group”, consisting of the Commissioner, the three directors and, before the 2015 restructuring, the Third Officer. The Commissioner’s Group met about once a week for informal meetings, which were not minuted, to share information with the aim of improving communications between the Commissioner and the directors.[180] Commissioner Dobson said that his day-to-day management and oversight of the directors was not exercised through the Commissioner’s Group, but by daily individual meetings and, more formally, at the Corporate Management Board.[181]
The Operational Directorates Co-ordination Board (the co-ordination board) comprised the directors and most of the senior officers and heads of department in the LFB’s two operational directorates. It comprised the heads of Operational Prevention and Response, Fire Safety Regulation, Operational Procedures, Operational Resilience and Human Resources and Development (the training department). The control room was not represented. Until 2015 the co-ordination board was chaired by the Deputy Commissioner, Rita Dexter; following the restructuring in 2015 it was chaired by AC Brown in his capacity as Director of Operations. The Commissioner was not a member of the co-ordination board and did not attend its meetings.[182]
The primary function of the co-ordination board was to provide a forum in which the two operational directorates[183] could discuss and co-ordinate their activities, identify risks to operational staff and identify and recommend training required in response to such risks.[184] Trends and lessons identified by the Operational Assurance department were brought to the co-ordination board for discussion. The co-ordination board would then select the most significant operational topics for development into paper or computer-based training.
In late 2016, the name of the co-ordination board was changed to the Operational Professionalism Board[185] but that had no effect on its working.
In the Phase 1 report, the chairman found various shortcomings in the LFB’s training, which were revealed in its response to the fire, both on the fire ground and in the control room.[186] In this phase of the Inquiry, therefore, we have examined the way in which the LFB identified training needs (particularly those arising from incidents), its approach to the procurement and provision of training and its systems for monitoring the effectiveness of training.
The LFB had a complex system for identifying the need for training and delivering training to staff at various levels. A process known as the dynamic and intelligent operational training (DIOT) process was central to the operation of that system. Its purpose, as described in Policy No. 825 (PN825), was to monitor operational, health and safety and training performance, to identify trends and provide mechanisms to support the maintenance of competence on the part of operational staff.[187] As Deputy Commissioner Dexter agreed, that somewhat complex description could fairly be summarised as learning from mistakes made in fighting fires and promoting good practice.[188] Its principal purpose, and that of the co-ordination board more generally, was to identify risks to operational staff and to provide appropriate training.[189] The process could also, in theory, result in the amendment of an existing policy or the introduction of a new policy, but PN825 described that outcome as rare.[190] Ensuring that the objectives of the process were achieved was the main responsibility of the co-ordination board.[191]
Central to the process were the arrangements for monitoring incidents and the creation of the associated database described in PN825. The database was used to record comments on the performance of operational personnel or the brigade as a whole during incidents and training.[192] Such comments, often referred to as “development points”,[193] typically emerged from meetings held after operational incidents or training exercises specifically to consider the quality of the response and the performance of the incident commanders.[194] PN825 made it clear that entries should be made on the database only in cases where the performance of an individual, team, piece of equipment or the organisation as a whole had fallen below the required standard or had exceeded expectations.[195]
Except in the case of monitoring officers, who were required to post comments on the database in certain cases, firefighters of all ranks could post comments if they wished to draw attention to something they considered to be of importance in relation to the operational response. (Comments made as a result of meetings to consider the performance of incident commanders were posted on the database in all cases.)
The Incident Management Policy group, which was part of the Operational Assurance directorate, was responsible for analysing the database and producing six-monthly reports to the co-ordination board identifying significant trends and matters that required attention.[196]
Although the system could be used by firefighters of all ranks, DC Dexter and Commissioner Cotton agreed that few firefighters made use of the opportunity to make comments.[197] One biannual incident monitoring report in 2014 shows that entries were made in respect of only 4% of the 47,105 incidents recorded[198] and it follows that 96% of incidents during that period generated no comments at all. The report indicated that those figures represented an increase on previous quarters, when the use of the system must have been even lower.
Commissioner Cotton and Dr Sabrina Cohen-Hatton, head of the Operational Review Team in June 2017, said that operational staff, especially incident commanders, saw development points as negative.[199] Ms Cotton also said that both firefighters and officers found it difficult to accept criticism of their operational performance[200] and Deputy Commissioner Dexter said that some staff had voiced fears that they might get into trouble if they admitted having done something wrong.[201]
Commissioner Cotton said that she saw no connection between the negative perception of development points and the less than enthusiastic use of the system.[202] On the other hand, Deputy Commissioner Dexter told us that the negative perception of development points was the main reason given for not posting comments.[203] That is the most plausible explanation we were given for the significant under-use of the system. The LFB did attempt to improve the use of the database by seeking to reassure staff that development points were not intended to be punitive and by informing officers of the importance of posting comments, but its efforts were unsuccessful.[204]
The low use made of the monitoring process and the very low proportion of incidents which gave rise to development points (even allowing for the fact that many of them were very minor) meant that the database was very narrow and could provide the co-ordination board with only a limited picture of operational trends or training needs. The process concentrated too much on identifying long-term trends, with the result that a serious problem disclosed by a single significant incident could be missed.[205] For example, the database entry for the Shepherd’s Court fire in 2016, a significant incident involving the spread of fire across the combustible facade panels of a high-rise residential block and a partial evacuation, failed to identify the spread of fire across external walls or the use of combustible panels as matters to be considered.[206]
Deputy Commissioner Dexter accepted that the incident monitoring process fundamentally relied on the willingness of individual officers on the ground to provide information and that, in the context of a falling number of incidents, the amount of information available to it was steadily diminishing.[207]
On receipt of a six-monthly database report, the co-ordination board considered whether any training was required in response to what it disclosed. Training was delivered primarily in the form of articles published in Operational News, the LFB’s internal information circular, some of which were accompanied by computer-based training packages. Indeed, Operational News and its associated training packages were the main focus of the co-ordination board’s work.[208] Commissioner Cotton estimated that only half to two thirds of the operational trends identified in the database reports were in fact chosen as subjects for articles in Operational News.[209]
The Incident Management Policy group was responsible for producing articles for publication in Operational News, although the articles themselves were drafted by experts from the relevant departments before being reviewed and approved by Operational Assurance.[210] They typically took the form of a summary of an existing policy, drawing firefighters’ attention to its contents. Babcock produced reports every six months, in conjunction with the Human Resources and Development department, telling the co-ordination board how the training it was providing had been, or was being, improved to support the topics covered in the previous edition of Operational News. In many of those reports Babcock simply stated that the topics in question were already adequately covered.[211]
Commissioner Cotton said that summarising an existing policy in Operational News did not amount to training but had been intended to raise awareness and provide personnel with links to the associated training delivered through fire stations.[212] Initial training was provided to firefighters by Babcock, but the subsequent development and maintenance of operational skills was mainly carried out at station level in accordance with the Policy No. 427 (PN427) by means of computer-based training packages and lectures delivered by watch managers, attendance at which was recorded on crews’ training records.[213]
Watch managers were not provided with any centralised training materials for their lectures (apart from the policies themselves); instead, it was the responsibility of each watch manager to develop their own lectures and deliver them to crews.[214] For at least five years preceding the Grenfell Tower fire watch managers were given no guidance on how to deliver training and there was no process to ensure that officers who provided training were competent to do so.[215] Station-based training was monitored by Training Review Information Officers, who were responsible for ensuring that training was provided and that training records were complete and accurate.[216] But we have seen no evidence that any assessment of the quality of station-based training was carried out by those officers or anyone else.
This station-based training was separate from the centralised training that was commissioned by the Human Resources and Development department (later known as the Training and Development department) and provided by Babcock. For ease of reference and consistency, we shall refer to the department simply as “the Training department”. The Training department made no contribution to the substance of station-based training and played no part in ensuring that adequate station-based training was provided.[217] Nor did the Training department have any process by which to ensure that station-based training was consistent with the training provided by Babcock, which the LFB’s Head of Training, Peter Groves, accepted created an obvious risk of injury.[218] Mr Groves said that responsibility for identifying and assessing any omissions from station-based training lay with the individual borough commanders to whom stations reported, but he accepted that, since 2012, borough commanders had not been trained in how to make such assessments.[219]
The Training department’s limited involvement in supporting, monitoring or assessing the quality of station-based training is surprising and difficult to justify. The importance of Operational News to the delivery of training meant that the LFB was heavily reliant on local crews, local station managers and particularly local watch managers for creating and providing the associated lectures. That clearly created a significant risk that the training that crews at different stations received differed in content and quality.
Commissioner Cotton accepted that articles in Operational News could never provide more than a high-level, cursory exploration of an operational topic.[220] She also agreed that the quality of station-based training depended entirely on the skills of individual watch managers.[221] The co-ordination board’s principal method of evaluating the effectiveness of that training was to see whether a particular problem featured in later incident monitoring reports.[222] Many of the reports considered by the co-ordination board indicated that it was difficult to teach some lessons, as evidenced by the fact that some problems kept recurring.[223] Although the reports occasionally noted improvements resulting from certain steps that had been taken (presumably because the number of development points relating to that topic had reduced), there was no system by which the co-ordination board could assess the effectiveness of articles published in Operational News or station-based training.[224] The co-ordination board’s approach, which lacked any active assessment of the effectiveness of its training interventions, was wholly inadequate. It was foreseeable that it might fail to identify or resolve significant problems and in any event could identify problems only after they had occurred with sufficient frequency or severity to be noted in one or more incident monitoring reports.
At a meeting held on 14 October 2013, the co-ordination board decided to carry out a fundamental review of the system, because it realised that the same shortcomings were repeatedly occurring. The review was to examine whether the right tools were available to the brigade for monitoring the effectiveness of training and what systems were used by other organisations. It was envisaged that it might lead to a review of the way in which the LFB responded to incidents. Ms Cotton, then AC Operational Assurance, was asked to lead the review.[225] In the event, however, it was not as fundamental or far-reaching as had originally been intended or as was required, and although it led to a number of recommendations, it did not result in any significant changes to the system for monitoring the effectiveness of training.[226] No one was able to explain why the stated aim of the review had not been met or why the opportunity to reform the existing arrangements had not been seized.[227]
In April 2012, the LFB engaged Babcock to provide centralised training to operational firefighters but retained responsibility for training non-operational officers, including the control room and the Fire Safety department. Shortly after being appointed as training provider, Babcock agreed to undertake a review of all the LFB’s training courses within the first three years of the contract. The LFB’s course review board, chaired by Director Reason, was responsible for considering and approving Babcock’s proposals.[228]
Although Babcock was responsible for creating and providing operational training packages, the LFB alone determined learning objectives and in practice provided much, if not all, of the expertise necessary for the production of the content. At all times it retained ultimate responsibility for training its staff and no training package could be provided by Babcock unless it had been approved by the LFB.[229] The systems and structures relating to the training provided by Babcock were entirely separate from those relating to station-based training.
Responsibility for managing the LFB’s relationship with Babcock lay with the Training department. The Training department had no role in identifying training needs, recommending new training or requesting changes to existing training. Those were the responsibility of other departments, known as “commissioning departments”. The Training department’s role was essentially administrative: it collated training needs and requirements received from other departments and organised the process by which they were ultimately translated into training by Babcock.[230]
The Training department had two teams. The Learning and Development Strategy team was responsible for managing the development of training packages and communicating with Babcock and the commissioning departments.[231] The Training Assurance and Business Relationship team was responsible for ensuring that Babcock provided the training that had been agreed and that it met the LFB’s learning and training objectives.[232]
Training was commissioned in accordance with a process known as the “training commissioning and alterations process” (TCAP). When a training requirement had been identified, the commissioning department completed a form identifying in broad terms what was needed.[233] Project managers in the Training and Professional Development team, in consultation with the commissioning department, then completed what was known as a “TCAP form” which built on the basic information provided in the training request by addressing practical aspects of both substance and implementation.[234] When the team was satisfied that it was correct, the form was submitted to a group consisting of representatives of both Babcock and the LFB’s Training department to check that the training would not have a detrimental effect on operational services.[235] Babcock could suggest additions or changes to training but did so only once in the period before the Grenfell Tower fire.[236]
The next stage of the process was the development of the substantive training. Babcock proposed and designed the content of the training package to meet the identified learning objectives, subject to the approval of the commissioning department.[237] Although it managed the commissioning process, the Training department did not play a part in designing the training itself.[238] Babcock usually produced three options for providing the training for consideration by the LFB, which then made a choice.[239]
When the training materials had been assembled, a pilot training course was developed (except for some computer-based training), which was attended by experts and representatives of the commissioning department to ensure that it met the LFB’s needs.[240] If the pilot course was considered satisfactory, it was necessary to obtain the commissioning department’s approval, confirmation from Babcock that the design was complete and approval from the Head of Fire Stations and the Training department for the provision of the training to operational staff.[241] At that point the training could be rolled out. Some training packages were either delayed or not released at all following the completion of a TCAP form.
A consistent theme of the evidence was that Babcock lacked the expertise required to develop appropriate training. As a result, the LFB frequently had to provide experts from within its own ranks to assist it, which was a significant drain on resources.[242] The problem was most acute at the start of the contract in 2012, particularly in relation to incident command training. It was therefore forced to rely on LFB officers to provide the necessary expertise, with the result that it was not always possible to implement much-needed changes to incident command training with sufficient urgency.[243] Babcock’s reliance on the LFB for expertise also delayed other areas of training, including training on the use of breathing apparatus and real fire training.[244]
Although Mr Groves considered that it was Babcock’s responsibility to secure the expertise it needed, he rightly accepted that, whatever its contractual arrangements with Babcock, the LFB ultimately remained responsible for ensuring that firefighters were adequately trained.[245]
A report by Ribband Starr Ltd, commissioned by the LFB after the Grenfell Tower fire, found that many within the LFB regarded the commissioning process as cumbersome and capable of causing significant delay in the design and delivery of new courses.[246] All the LFB witnesses who gave evidence about training were of that view.[247] We agree with their assessment.
We were told that all training courses referred to in the annual statement of training requirements produced by the Training department were audited separately at least once a year by the LFB and Babcock and that the results were discussed at monthly meetings between Babcock and the Training department to decide whether any change to a particular training course was needed.[248] The Inquiry has not seen any evidence of audits or discussion of their findings. In particular, there is no evidence that audits resulted in the creation or amendment of any training packages. If audits were carried out, they appear to have had no effect on the content of training.
PN825 refers to four levels of evaluation used by the LFB to assess the effectiveness of training. Level 1 involves the use of questionnaires seeking the opinions of those who have attended courses,[249] Level 2 gauges what trainees have learnt, Level 3 assesses whether trainees have been able to apply their new skills and knowledge to the workplace, and Level 4 considers the effect of the training on the organisation as a whole.[250] We were told that training courses, apart from computer-based training, had been subject to Level 1 evaluation but that no formal Level 3 or Level 4 evaluations had been carried out.[251]
There was no system in place for evaluating the performance of staff who had attended training courses by reference to previously agreed criteria. Once a training package had been developed by Babcock and approved by the commissioning department it was assumed to be suitable.[252] That might have been a reasonable approach if the LFB had implemented adequate arrangements to review the effectiveness of training courses, but it is plain that it had made no such arrangements. The approach was particularly unsound in circumstances where there was no process at all by which the Training department was able to review the overall effectiveness of a training programme.[253]
We have been left with the clear impression that, instead of adopting a system which measured the effectiveness of training by reference to previously agreed criteria, the LFB simply waited to see what, if any, problems subsequently arose at incidents. Such an approach might or might not reveal any deficiencies in training, but if it did, it was by then likely to be too late. The obvious weaknesses of that approach were aggravated by the fact that, as the number of incidents declined, progressively less confidence could be placed in a system that relied on problems being identified at incidents.[254]
The procedure adopted by the LFB for commissioning training in the years leading up to the Grenfell Tower fire placed much emphasis on ensuring that the right courses were produced and that training did not interfere with operational requirements. Both were laudable aims. However, the process was very cumbersome and inevitably led to excessive delay in providing new courses. There was also a disturbing absence of any system for evaluating the effectiveness of courses once they had been introduced. At a local level too much responsibility was placed on watch managers to devise and deliver training, with insufficient support and oversight. Since the quality of training at that level depended to a considerable extent on the skills of individual watch managers, the quality was bound to be variable.
In the Phase 1 report the chairman found that the incident commanders who were present during the early stages of the fire had not received sufficient training to enable them to understand the nature of the fire that confronted them and how it was likely to develop. We do not think that the deficiencies in the system for commissioning training or the arrangements for delivering training at station level that we have identified were responsible for that shortcoming, although we cannot be confident that, if there had been sufficient understanding of the need for training in the risks of cladding fires in high-rise buildings, it would have been delivered promptly and effectively. In the next chapter we examine why the LFB failed to ensure that those who acted as incident commanders were properly trained for the task.
It became apparent during the course of the Grenfell Tower fire that few, if any, of those who were called upon to act as incident commanders in the early stages of the fire had received training in how to recognise a fire in the external wall of a high-rise residential building or to understand its likely consequences. Nor had they received any training in the principles of evacuation from high-rise residential buildings when a “stay put” strategy was no longer tenable, in how to decide whether evacuation was necessary or in how to carry it out safely and efficiently.[255] It was therefore necessary for us to examine the way in which the LFB trained those who might be expected to assume the responsibility of incident commander and in doing so we must assess its response to the recommendations on incident command made by the coroner in March 2013, following the Lakanal House inquests.
There appears to be little doubt that before the Lakanal House fire in July 2009 only a small number of officers in the LFB were aware of the dangers posed by combustible materials when used in external walls of buildings or could recognise and understand the significance of a fire of the kind that broke out in Grenfell Tower in June 2017. Those who could and did were almost entirely confined to the Fire Safety department and did not include any of those who could be expected to act as incident commanders.
The Lakanal House fire should have changed that for ever, because operational firefighters at many levels witnessed at first hand the effects of fire spreading across an external wall as a result of the presence of combustible panels. They also witnessed the extensive loss of compartmentation caused in part by the spread of fire both externally and internally, the latter as a result of the use of unsuitable materials in the refurbishment of the interior, in particular some of the corridors. That should have been enough to prompt the LFB to take urgent steps to ensure that in future incident commanders were able to recognise a rapid loss of compartmentation and the spread of fire on the exterior of a building, if it occurred, and knew how to respond, almost certainly by evacuating the whole or part of the building. However, the need for such training should have been put beyond doubt by the coroner’s rule 43 letter, written over three years after the fire.
In her rule 43 letter to the LFB the coroner recommended that consideration be given to the training of incident commanders to enhance their performance in a number of respects, including their ability to understand and react quickly to changing circumstances and to anticipate that a fire might behave in a manner inconsistent with the compartmentation principle.[256]
AC Cotton, who was head of the department responsible for incident command policy and training at the time, was asked to respond to the coroner’s recommendations.[257] Her suggested response, which was ultimately adopted by the Commissioner’s Group, was that the LFB should work with Babcock to ensure that all the points raised by the coroner were covered in its current review of incident command training in the period up to 2015 and to create a case study training package which would teach the lessons to be learnt from the Lakanal House fire and other high-rise fires, such as the one at Shirley Towers. The suggestion ultimately resulted in the Lakanal House case study, to which we will refer later. However, as noted there, the case study did not provide adequate training for incident commanders facing a widespread failure of compartmentation of the kind experienced at Lakanal House, nor did it specifically address the coroner’s incident command recommendations.[258]
The LFB accordingly instructed Babcock to incorporate the coroner’s recommendations into its review of incident command training, which by then was already in progress. In addition, the LFB instructed Babcock to conduct a separate review to confirm that all the coroner’s recommendations relating to incident command were fully covered by existing training courses.[259] That review was carried out in mid-September 2013 and the results were provided to the Operational Assurance department.[260] The results of Babcock’s review were not considered by Director Reason.[261]
Babcock concluded that the existing training explicitly or implicitly covered all the areas identified by the coroner. Some were the subject of both theoretical and practical training; in other cases the extent to which the areas identified by the coroner were covered and the performance of trainees assessed depended on the exercises they undertook. Babcock recommended that the LFB revise its existing exercises in order to implement the coroner’s recommendations and identified 16 exercises which could provide starting points for new exercises which would fully implement those recommendations.[262]
In Chapter 74 we describe how in June 2013 LFEPA had set up a working group to monitor the LFB’s response to the Lakanal House fire. The LFB’s report to the working group on 30 September 2013 gave a different impression from that indicated by Babcock in its review. It said that Babcock had confirmed that all the coroner’s recommendations were covered by the existing training on incident command, although there might be opportunities for emphasising the experience obtained from the Lakanal House fire in some cases.[263] That was inaccurate. Babcock had concluded that further work was required on the existing exercises and had identified the fact that some candidates for incident command might not have taken part in any of the relevant exercises.[264] In such cases they would not have received any training on matters covered by the coroner’s recommendations. However, the fact that some incident commanders would not receive training on matters falling within the coroner’s recommendations was an important fact that was omitted from the LFB’s report.
In the LFB’s report to the working group in November 2013 that task was marked as having been completed. For reasons explained below, that too was inaccurate, since the work was by then far from complete.[265] Director Reason accepted that the reports did not disclose that Babcock had found that some individuals were not receiving training in the areas identified by the coroner, that incident command training therefore required enhancement, and that the work to develop training exercises was continuing.[266] He said that he had relied on the information he had received from the co-ordination board’s monitoring of the response to the recommendations and that it had been the responsibility of AC Cotton and her commissioning department to ensure the accuracy of the information.[267] He told us that he had provided the working group with the information that AC Cotton’s department had collated for the co-ordination board.[268]
AC Cotton considered that the reports were misleading but said that she was puzzled why the tasks had been marked as completed, because at that stage they were very far from completing the enhancement to the training programme that Babcock was going to undertake.[269] She said that she could not recall ever having seen a report to the co-ordination board indicating that the task had been completed; if she had, she would have challenged it.[270]
AC Cotton disputed Director Reason’s evidence that he had depended on reports emanating from the co-ordination board. In her view, he had a far better understanding of the position than his evidence suggested. She thought he had been fully aware that a number of tasks were outstanding because he was a member of the co-ordination board and had seen the progress reports. She said that the reports on incident command training had been discussed at length in directorate management board meetings and in her meetings with him. She added that Director Reason was not the sort of person who would accept what was given to him at face value. He would explore the detail.
In January 2014 Director Reason asked Adrian Bevan, a health and safety manager in the LFB,[271] to provide him with a document to support the paragraph in the report to the working group which stated that all seven recommendations were adequately covered by the existing training exercises. Having made some enquiries, Mr Bevan reported that the position was not as clear as had been thought because there had been some confusion between current training exercises and the new exercises that Babcock were developing. At that point, if not before, therefore, Director Reason must have been aware that the position was not as had been reported to the working group. However he did not attempt to correct the reports.[272] Director Reason should have ensured that his reports to the Lakanal House Working Group accurately reflected the delay to the new incident command training programme.
Babcock’s initial proposal to revise and refine 16 command training exercises was not carried out. First the number was reduced to six and in the end only one, the Holcroft House exercise, was developed. The reasons for that are not entirely clear.[273]
The Holcroft House exercise became available in 2016. It centred on a fire at a high-rise residential block in Battersea which was undergoing decorative and remedial building works. The overview of the exercise described it as increasing in complexity to involve persons reported as trapped and needing rescue, fire survival guidance calls, significant fire growth and the need for mass evacuation, compounded by the hazards and risks associated with the remedial building works. It was intended to create significant challenges for crew managers and watch managers. A detailed description of the exercise and its potential variations disclosed that it involved only two fire survival guidance calls (at the Lakanal House fire there had been five) and the spread of fire from the original compartment only to the communal corridor, rather than to other floors. The training guide stated that trainees were expected to consider partial or full evacuation of the block, but there was nothing in the course materials designed to help them understand why they might need to consider an evacuation or how they might organise one.[274] For all those reasons, as Director Reason accepted, that particular training package was not an adequate response to the coroner’s recommendations.[275] Director Reason was not involved in the development of that package but did have ultimate responsibility for changes to the LFB’s incident command training in response to the coroner’s recommendations until his retirement on 2 January 2015.
There was conflicting evidence about whether it was intended to make the Holcroft House exercise available to all potential incident commanders,[276] but in the event, it was restricted, for reasons which are not clear, to Level 1 incident commanders (crew managers and watch managers), rather than being provided to all four levels of incident commander as had been envisaged by Babcock’s initial proposal.[277] As a result, a significant number of incident commanders did not receive the training which had been designed to implement the coroner’s recommendations.
Director Reason told us that the LFB was likely to have partially implemented the coroner’s recommendations before August 2016 through Babcock’s making simple adjustments to existing courses and by changing the procedures for assessing suitability for senior officer positions.[278] However, apart from a report which stated that assessments of suitability for incident command covered the challenges of managing incidents affecting high-rise buildings,[279] there was no contemporaneous evidence that changes to training courses or to the assessment procedures had been made to reflect the coroner’s recommendations. If changes of that kind had been made, we think they would almost certainly have been recorded, if only informally. We are therefore unable to accept what Director Reason said on that matter.
We have no doubt that the LFB intended to incorporate the coroner’s seven incident command recommendations into Babcock’s review of incident command courses,[280] which should have ensured that from 2015 the recommendations were reflected in new incident command courses. However, the evidence clearly shows that they were not considered in any detail by either Babcock[281] or by the LFB during its review of the courses.[282] That was a significant failing by the LFB, which should have ensured that the lessons to be learnt from the Lakanal House fire were at the heart of the review that it had instructed Babcock to undertake.
Director Reason told us that the LFB’s Course Review Board and Babcock’s review of the training courses were separate from the recommendations of the Lakanal House Board and those made by the coroner.[283] Although they may have had separate origins, however, it was clear that the LFB intended to incorporate the coroner’s recommendations into Babcock’s review of training, as indeed had been conveyed to the coroner.[284] That was also confirmed by AC Cotton, who was involved in the review of training courses relating to incident command that was overseen by the Incident Command Project Board.[285] Both AC Cotton and Director Reason could and should have ensured that the incident command recommendations were taken into account in that course review.
Even if the new incident command courses adequately reflected the lessons to be learnt from the Lakanal House fire, most of them had not been made available to operational personnel by the time of the Grenfell Tower fire. Courses for Level 1 incident commanders were made available between 2016 and 2017, but courses for Level 2 (station managers and group managers), Level 3 (Deputy Assistant Commissioners) and Level 4 (Assistant Commissioners and above) were either yet to be made available or were still being worked on at the time of the Grenfell Tower fire.[286] That was almost three years after the LFB had received Babcock’s report on its review of training courses and over two years after the revisions should have been completed.[287] AC Cotton described that rate of progress as “worse than slow”. She said that she had regularly reported her frustrations and serious concern about the lack of progress that was being made.[288]
We heard forthright evidence from a number of witnesses about the difficulties that Babcock had experienced in providing incident command training, which they attributed to its lack of expertise (which required a greater contribution from the LFB than had been expected), delay in creating training packages and difficulty translating proposals for training into courses.[289] AC Cotton described Babcock’s inability to develop incident command training as one of her greatest frustrations. She said that the LFB could not take back control of training because it had lost the teams that it had previously relied on for developing courses.[290]
Babcock’s lack of expertise clearly contributed to the significant delay in the development and release of the revised incident command training. Peter Groves told us that it should normally take no more than a year to produce a new course but that the complexity of training for incident command and Babcock’s lack of expertise had delayed the process. He agreed, however, that a lapse of three years between the receipt of the coroner’s recommendations and the release of the Holcroft House exercise was unduly long. He attributed the delay to Babcock’s lack of expertise,[291] but the LFB was ultimately responsible for the protection of life and property and of its own staff and had a duty to ensure that adequate training was provided to its crews for that purpose. Although we heard evidence that Commissioner Dobson had raised the delay with the chief executive of Babcock, they appear to have concluded that neither Babcock nor the LFB was at fault and to have confined themselves to repeating the importance of complying with the coroner’s recommendations.[292] The discussions had little or no effect on the delay. We do not think that the steps taken by the LFB to remedy the problems with Babcock were sufficiently robust.
Some senior LFB officers thought that the coroner’s recommendations did not require any substantive revisions to the LFB’s existing incident command training. For example, Commissioner Dobson told us that the LFB had not needed to revise its incident command training; all that was needed, he thought, was for the seven recommendations to be enhanced and properly embedded.[293] Similarly, AC Cotton said that the recommendations were not inconsistent with existing policy and procedures[294] and Director Reason did not think that the recommendations reflected the existence of a systemic problem.[295] We think that views of that kind held by senior officers are likely to have undermined the importance attached to the training packages and to have added to the delay.
Another aspect of incident command training that was under development at the time of the Grenfell Tower fire was a programme of continuing assessment of competence to undertake incident command, known as incident command revalidation. The purpose of the programme was to ensure that operational officers of crew manager rank and above maintained the required level of competence as incident commanders throughout their operational careers. That contrasted with the position under the LFB’s incident command training arrangements existing at the time of the Grenfell Tower fire, under which competence to undertake incident command was assessed by way of an exercise undertaken only when an officer was being considered for promotion. Under those arrangements no further assessment took place unless and until that officer was being considered for further promotion. None of the continuing incident command training that existed immediately before the Grenfell Tower fire contained any form of assessment, and officers who undertook that training continued in their existing rank regardless of their performance during training.
Proposals for an incident command revalidation programme had first been put forward to the Commissioners’ Group by Dr Sabrina Cohen-Hatton, then a DAC and the LFB’s Head of Development, in a report dated 17 November 2015.[296] She referred to the declining number of incidents in the years preceding the report, which had resulted in a reduction in operational experience across the board and, in particular, a reduction in the number of opportunities for officers to undertake command roles. Her department had consulted five other fire and rescue services, all of which were operating a revalidation system of some kind involving a formal assessment of competence to undertake incident command roughly every 18 to 24 months.[297]
The report to the Commissioners’ Group also referred to the remarkably low pass rates for the LFB’s existing incident command promotional exercises, in which just 25% of station managers and group managers and 36% of Deputy Assistant Commissioners were successful. Dr Cohen-Hatton said that the low pass rates were likely to be explained by the fact that candidates received no training in how to command an incident of the scale and complexity that they were required to tackle as part of the promotional exercise, meaning that the first time that many of them had encountered such an environment was at the assessment itself.[298]
The report recommended a revalidation programme consisting of three elements: a test to assess levels of technical and procedural knowledge, another test to assess command skills by means of an incident command exercise, and the demonstration by means of a continuing professional development (CPD) log that incident command skills had been consistently and effectively applied on the incident ground. Dr Cohen-Hatton proposed that the three elements should be assessed every two years, with provision for additional training to be undertaken by those who scored below a minimum threshold, or, in the most serious cases, removal from operational duties.
The proposed revalidation programme was developed separately from the work being carried out on the coroner’s recommendations, but its implementation depended on the delivery of the new incident command training exercise being developed as part of Babcock’s wider review. Since the LFB lacked the necessary resources to provide and assess a separate exercise just for the revalidation programme, the incident command exercise to be used for the revalidation process had to form part of the new incident command refresher training.[299] The delay in the development of the new course therefore delayed the progress of the incident command revalidation programme.
The original timetable for the revalidation programme had been set out in a report to the Corporate Management Board dated 16 December 2015, which recorded that the knowledge tests and the incident command exercise were to be launched in April 2016 and the use of CPD logs in April 2017.[300] However, by the time that Dr Cohen-Hatton reported to the Corporate Management Board on 8 June 2016 those dates had been pushed back to some indeterminate time in 2016 or 2017, in the case of the knowledge tests and incident command exercise, and 2017 or 2018 in the case of the CPD logs.[301] At a meeting of the Incident Command Project Board on 23 February 2017, Dr Cohen-Hatton expressed her concern that the implementation of a revalidation programme was being pushed back as a result of the delay in the broader review of incident command training.[302] A briefing note prepared for the Corporate Management Board in March 2017 stated that pilots of some of the knowledge tests would be carried out in May 2017 and indicated that a draft policy was in the final stages of development.[303] By that stage Dr Cohen-Hatton’s team had done most of what they could do pending the delivery of the incident command training being developed in response to the broader review.[304]
The revalidation programme had still not been implemented at the time of the Grenfell Tower fire, nor by the time of the inspection of the LFB by Her Majesty’s Inspectorate of Constabulary and Fire and Rescue Service (HMICFRS) in May and June 2019, which identified the lack of any revalidation system as a cause for concern requiring immediate action by the LFB.[305]
In the Phase 1 report, the chairman found that the absence of any training for incident commanders in how to recognise the need for evacuation reflected a failure to recognise the risk of fire taking hold on the outside of modern buildings.[306] He expressed the view that it was a surprising failure, given the long history of fires involving cladding on high-rise buildings both in this country and abroad, a history of which some people within the LFB had been aware for some time.[307]
Before the Lakanal House fire in July 2009, there had already been two significant fires in the UK which had involved the extensive spread of fire through combustible external panels. On 5 April 1991, a fire was started deliberately in a rubbish compound outside Knowsley Heights, an 11-storey residential building in Liverpool. The fire spread rapidly through a 90mm gap between the building’s concrete outer wall covered with rubberised paint and rain screen panels which had recently been installed. The fire spread to the highest floor and seriously damaged the outer walls and windows of all the upper floors.[308]
On 11 June 1999, a fire started on the fifth floor of Garnock Court, a 14-storey residential building in Irvine, Scotland. The fire spread rapidly to the higher floors through a vertical strip of external cladding, resulting in one fatality.[309]
The fire at Garnock Court was the subject of a report by the Environment, Transport and Regional Affairs Committee entitled Potential Risk of Fire Spread in Buildings via External Cladding Systems.[310] The report, published in December 1999, drew attention to the risk of the unexpectedly rapid spread of fire through cladding systems, which could lead to disproportionate difficulties in firefighting and a shorter period available for escape from the building, potentially endangering life.[311] The committee concluded that the evidence before it did not suggest that the majority of external cladding systems in the UK posed a serious threat to life or property in the event of fire, but went on to say that, notwithstanding that conclusion, it did not believe that it should take a serious fire in which many people were killed before all reasonable steps were taken towards minimising the risks. It recommended that all external cladding systems be required to be either entirely non-combustible or proved through full-scale testing not to pose an unacceptable level of risk from the spread of fire.[312]
Apart from a passing reference to the Garnock Court fire in a presentation on the spread of fire across the facades of tall buildings created in 2016, the LFB failed to create any training materials which communicated to operational staff the key lessons to be learnt from those two fires. Deputy Commissioner Dexter said that she had been aware of the Knowsley Heights and Garnock Court fires during her time at the LFB position;[313] Commissioner Dobson said that he had been aware of the Knowsley Heights fire but not the Garnock Court fire.[314] Both agreed that those fires contained lessons for the LFB.[315] Commissioner Dobson’s recollection was that the fires had been considered by the Operations and Fire Safety departments, which had concluded that the lessons from those incidents had already been learnt by the LFB or were not relevant to it.[316]
Also on 23 March 2009, AC Stephen Turek, then in charge of Fire Safety Regulation, wrote to London Boroughs and social housing landlords about fire safety in social housing.[317] In his letter he said that it had been written in the light of a number of recent fires in social housing blocks,[318] and drew attention to several aspects of construction that could present dangers. They included the following:
The letter had apparently been based on fire investigation reports relating to premises where such defects had been noticed following inspections by fire safety regulation officers.[319]
The evidence as a whole, but particularly the letter of 23 March 2009, shows that by that date some senior officers within the LFB had become aware:
As the chairman explained in Chapter 8 of the Phase 1 report, Lakanal House was a high-rise residential tower block in Camberwell, South London. On 3 July 2009, a fire broke out in a flat on the ninth floor of the building. Within 30 minutes it had spread down to the fifth floor and up to the twelfth floor as well as to communal areas, including corridors and the building’s single staircase. Six people lost their lives and 15 people were taken to hospital suffering from smoke inhalation. The incident involved a widespread failure of compartmentation and extensive spread of fire and smoke.[320] The fire was able to spread across the external wall (both upwards and downwards) as a result of the presence of combustible window panels that did not comply with the Building Regulations.[321] The incident was also characterised by an unusually high number of fire survival guidance calls (five in total),[322] poor communication between the control room and the incident ground, difficulties with radio communications generally and confusion among firefighters about the layout of the building and the locations of flats.[323]
The Lakanal House fire in July 2009 was a watershed moment for the LFB and was undoubtedly the most significant residential fire in which it had been involved in the years immediately preceding the Grenfell Tower fire. It is of particular importance because it marked a milestone in the history of the LFB’s response to fires in high-rise residential buildings and the handling of emergency calls. It prefigured in many respects the Grenfell Tower fire some eight years later and it is therefore appropriate to consider how the LFB responded to the experience and the extent to which it learned from it.
In October 2009, Commissioner Dobson set up the Lakanal House Board to oversee the LFB’s internal investigation into the fire and its response to it. It was chaired by the Commissioner and attended by a wide range of senior officers. The board was responsible for identifying the lessons to be drawn from the incident and for making any recommendations for organisational change that were thought necessary.[324] It met monthly and provided a forum for senior officers to discuss matters arising from the LFB’s investigation into the fire, to agree a response and to allocate responsibility for action to relevant departments and officers.[325]
The Lakanal House Board identified 34 steps that could be taken to improve the LFB’s operational response. They were set out in an action plan agreed at a meeting of the Board on 15 September 2010. Each step was assigned to an officer who was responsible for its implementation.[326] At subsequent meetings those officers provided regular reports on progress which were reflected in a rolling plan of action.[327] The 34 steps became known internally as the “pre-inquest actions”, or simply “pre-actions”. They covered a wide range of subjects, from the development of a policy relating to the risk of falling cables to writing to the government to obtain clarity on aspects of national guidance. They included a review of the LFB’s existing policies on firefighting in high-rise buildings and the management of emergency calls. Although some are of no relevance to our investigations, others are of central importance, such as the review of the LFB’s policy on firefighting in high-rise buildings and the provision of training to control room officers in handling fire survival guidance calls. However, the pre-inquest actions failed to include any response to what should have been the principal concerns arising from the Lakanal House fire, namely, the widespread failure of compartmentation and the spread of fire across external walls due to the use of combustible construction materials.
In September 2012, more than three years after the fire and in preparation for the Lakanal House inquests, Commissioner Dobson asked the Operational Assurance department, then headed by AC Cotton, to review the pre-actions to identify those which had been completed and those which had not.[328] Director Reason (to whom AC Cotton reported) delegated the task of carrying out the review to GM David Lindridge,[329] subject to the oversight of AC Cotton.[330]
GM Lindridge understood that his review was to involve no more than identifying which pre-actions had been carried out and which had not. He did not express a view on whether the actions taken were sufficient to meet the expectations of the board; he simply described the steps that had been taken so that others could make that assessment for themselves.[331]
In January 2013, GM Lindridge produced a report of his findings entitled Review of the Lakanal Action Plan (the Lindridge Review).[332] He found that 16 of the 34 tasks were still being worked on in one way or another and was unable to confirm that another 13 had achieved their expected outcomes.[333] GM Lindridge attached to his report a list of the pre-actions together with his findings on each of them. He also set out a list of his key findings in relation to ten of the pre-actions for the attention of the Commissioner’s Group. Most of them related to the control room.
GM Lindridge produced a revised version of his report in November 2013, in which he found that 8 actions had still not been completed (although in all but one of those cases the LFB was awaiting action by another organisation).[334] They included actions concerning the training of control room supervisors, pre-planning and correspondence with the government relating to aspects of fire safety.[335]
After receiving the Lindridge Review, neither AC Cotton nor anyone else appears to have considered whether the implementation of the Lakanal pre-inquest actions had been effective. Commissioner Cotton said that she had not been sufficiently qualified in a number of the areas being audited to express an opinion. In her view, it was the function of the Lakanal House Board to satisfy itself that the work had been done. She did not see it as part of her role as Head of Operational Assurance to be concerned with the detail of the actions referred to in the Lindridge Review.[336]
In the event, the Lindridge Review was never presented to the Lakanal House Board, which held its last meeting in September 2013 (though it was never formally disbanded). Commissioner Dobson said that his intention had been to have a final meeting formally to review and accept the revised Lindridge Review, but that it had been overlooked.[337] Nor was the Lindridge Review ever presented to the Lakanal House Working Group, referred to below, because the working group was directing its attention to the steps required in response to the findings made by the coroner.[338]
Although Commissioner Dobson said that responsibility for overseeing the progress of outstanding pre-inquest actions had been taken over by the co-ordination board,[339] we have seen no evidence of any such oversight in the minutes of its meetings. The Lindridge Review was, however, circulated to the Commissioner’s Group and discussed at a meeting in November 2013.[340] Director Reason’s recollection was that he and Deputy Commissioner Dexter had each accepted responsibility for the outstanding actions that fell within their respective directorates.[341]
After the Lakanal House Board effectively ceased to exist in September 2013, the LFB was left with no means of ascertaining whether the outstanding pre-inquest actions had been completed. Nor did it carry out any systematic inquiry to find out whether the work that had been done had been successful in making good the deficiencies the fire had uncovered. As a result, by 14 June 2017 significant steps that were relevant to dealing with the hazards that were later to confront the LFB at Grenfell Tower had not been taken. The LFB’s failure effectively to oversee the progress and completion of the changes in training and procedure it had identified as necessary in the light of the Lakanal House fire was a significant failing which prevented it from responding more effectively to the fire at Grenfell Tower.
Commissioner Cotton told us that monitoring the work on the Lakanal pre-inquest actions had not been the responsibility of the Operational Assurance department.[342] Although that may be true, it is unfortunate that the department responsible for ensuring the operational effectiveness of the LFB (and with learning from significant incidents) did not have, and did not seek, that responsibility, especially as no other department of the LFB did. Operational Assurance was the department to which the Commissioner had assigned responsibility for the review of the 34 pre-inquest actions in the first place and Commissioner Dobson should have ensured that there was no doubt about where responsibility for overseeing the implementation of the Lakanal pre-inquest actions lay. Ms Cotton had also been a member of the Lakanal House Board and she continued to sit on the co-ordination board, two key boards attended by the heads of service responsible for implementing the various changes. The Operational Assurance department was best placed to oversee the necessary changes, with the assistance of relevant experts where required, and to monitor the progress of any that remained outstanding. The Commissioner’s failure to assign responsibility clearly to the Operational Assurance department was a significant error.
There is no evidence that the LFB subsequently reviewed the 34 pre-inquest actions in the light of the Lakanal House coroner’s recommendations to see whether further changes might be required.[343]
The Lakanal House inquests were conducted by Her Honour Frances Kirkham CBE between January and March 2013. The coroner heard evidence from a number of LFB witnesses, including Commissioner Dobson.
Rule 43 of the Coroners Rules then in force allowed the coroner to make such recommendations as she considered necessary, based on the evidence heard during the inquest, to eliminate or reduce the risk of further deaths. On 28 March 2013, she sent Commissioner Dobson a letter pursuant to that rule (a rule 43 letter).[344] She also wrote to the Department for Communities and Local Government, the London Borough of Southwark and the Fire Sector Federation.
In her letter to the Commissioner the coroner acknowledged the work that the LFB had already carried out and recommended further action in five areas: public awareness of fire safety, visits made pursuant to section 7(2)(d) of the Fire and Rescue Services Act 2004, incident command, the control room, and communications. The substance of those recommendations will be considered in later chapters.
Following receipt of that letter, Commissioner Dobson instructed Director Reason to put together an action plan in response to the coroner’s recommendations.[345] In April 2013, Director Reason held a meeting with the heads of service responsible for the activities in question and asked each of them to produce a draft plan of action on the recommendations affecting their areas of responsibility.[346] Draft plans, referred to internally as “pro formas”, were produced by four heads of service, AC David Brown (Head of Operations, Procedures and Response), AC Stephen Turek (Head of Fire Safety Regulation), AC Dany Cotton (Head of Operational Assurance), and AC James Knighton (Head of Operational Procedures). They contained an analysis of the recommendations and proposed responses.[347] The pro formas were submitted to the Commissioner’s Group, which used them to draft the LFB’s response to the coroner’s letter.[348] That response was discussed and approved at a meeting of the Commissioner’s Group and the heads of service on 14 May 2013. The meeting was not minuted, but Director Reason’s recollection was that it had been concerned principally with the Commissioner’s review of the proposals and the time required to implement them.[349]
On 23 May 2013, Commissioner Dobson sent the LFB’s response to the coroner.[350] The letter set out the action which the LFB proposed to take in response to each recommendation and the time within which it would be completed. The Commissioner estimated that all the proposed actions would be completed by the end of 2013.
Responsibility for overseeing the progress of the steps that the LFB proposed to take was allocated to the co-ordination board and the Lakanal House Working Group.[351] (One of the co-ordination board’s existing functions was to monitor the progress of proposals for responding to rule 43 recommendations.)[352] At a meeting of the board on 3 June 2013 it was agreed that AC Cotton would develop a plan to monitor the progress of the response to the coroner’s recommendations.[353] A consolidated plan combining the response to the coroner with the LFB’s reaction to some rule 43 recommendations made by the Hampshire coroner following a fire at Shirley Towers in Southampton in which two firefighters had died was therefore produced for a meeting of the co-ordination board on 4 July 2013.[354]
Commissioner Dobson told us that he took personal responsibility for overseeing the response to the coroner’s letter, which, in addition to his role on the working group, he exercised in the course of meetings with individual directors and through the Commissioner’s Group.[355]
Overall, the response of the LFB to the Lakanal House fire was slow and ineffective. Although it soon established a process for identifying the lessons to be learnt and the steps needed to implement them, it took the best part of a year for it to identify those steps, several of which had not been implemented by the time that the first Lindridge Review was delivered two years later. Some had still not been implemented by the time that GM Lindridge produced his revised review in November 2013. The Lakanal House Board appears to have been allowed to lapse without any proper consideration of the extent to which the recommendations had been implemented, much less whether they had been successful. In our view, senior officers failed to provide the energetic and effective response that was required to an incident of such significance, for which Commissioner Dobson must bear primary responsibility.
The Lakanal House Working Group was established by LFEPA in June 2013 to review and oversee the LFB’s actions following the fire at Lakanal House and to provide regular information and any additional recommendations to LFEPA’s Strategy Committee.[356] It consisted of three elected members of the authority, Valerie Shawcross, Maurice Heaster and Peter Truesdale.[357] The working group was intended to provide political oversight, scrutiny and accountability for the LFB’s response to the coroner’s recommendations.[358] Although membership of the working group was formally limited to the three elected members, its meetings were also attended by Commissioner Dobson, Deputy Commissioner Dexter, Director Reason and other senior LFB officers as required in order to provide information on progress and answer members’ questions.
The outstanding pre-inquest actions were never brought to the attention of the working group, nor did it receive a copy of the Lindridge Review. When Director Reason was asked whether the working group might have benefited from seeing the review or from being told about the items that remained outstanding, he said that the elected members would probably not have wanted that level of information.[359]
Director Reason was responsible for presenting a report on the progress of the response to the coroner’s rule 43 letter at each meeting of the working group and reporting the current position in each case.[360] He said that his reports had been based on those that had been provided to the co-ordination board, presented in a slightly different way.[361] In reality, the difference was more than slight. The reports submitted to the working group did not provide its members with an accurate summary of the LFB’s incomplete progress in responding to the rule 43 letter. Most notably, as we have set out in detail in Chapter 72, some reports provided to the working group were misleading because they indicated that important changes to incident command training had been completed, when that was far from the case.
The Lakanal House Working Group met six times between July 2013 and March 2014. LFEPA’s Strategy Committee was told about the LFB’s actions on only two occasions, once in November 2013,[362] when work was still continuing, and once in July 2014.[363] That was clearly at odds with the working group’s objective of providing information to the Strategy Committee regularly.[364]
At its meeting in July 2014, the Strategy Committee received a report from Deputy Commissioner Dexter and Director Reason. The report summarised the LFB’s work in response to the coroner’s recommendations, recorded that the members of the working group were satisfied that they had fulfilled its original purpose and recommended that it be wound up.[365] That recommendation was accepted and the working group was formally closed. However, the report failed to disclose that a number of important items remained outstanding and the closure of the working group gave the misleading impression that all the proposed changes had been made.
Director Reason said that he had not intended to mislead the Strategy Committee and that it had not been the purpose of the report to rehearse all the information that had been put before the working group, merely to give a flavour of the subjects that had been covered.[366] He also told us that the members of the working group had been less interested in the details of operational procedures, policy and training than in wanting to understand broadly what the LFB had been doing.[367] We found his explanation unconvincing. The report presented to the Strategy Committee was not merely short on detail; it was, for the reasons summarised above and set out in greater detail in Chapter 72, misleading. With the closure of the working group, the report also ended active scrutiny by LFEPA of the outstanding responses to the rule 43 letter.[368] Director Reason said that it had not been the LFB but the members of the working group who had decided that it should be closed down, because, based on the information they had been given, they were satisfied that they had completed what they had set out to achieve.[369] However, for the reasons we have given, that information was incomplete and therefore misleading. Although we accept that was not Director Reason’s intention, it was the practical effect of providing incomplete reports.
In fact, certain steps identified by the LFB as necessary in response to the coroner’s rule 43 letter remained outstanding at the time of the Grenfell Tower fire. In July 2014, the Lakanal House Working Group could and should have been given an accurate summary of the extent to which the LFB had implemented the various changes required in response to the Lakanal House fire. If it had been given that information, it would have been obvious to the working group that the LFB had not responded fully to the coroner’s recommendations. By failing to provide it the LFB denied members of the working group the opportunity to challenge the Commissioner about the LFB’s dilatory and incomplete progress and, more broadly, prevented them exercising their public duty of holding the LFB to account. We are satisfied that the closure of the working group and the consequent lack of active scrutiny by LFEPA contributed to the LFB’s failure to implement the coroner’s recommendations fully. That lack of scrutiny was compounded by the LFB’s failure to complete its own pre-inquest actions. Not only did the LFB fail to learn from the Lakanal House fire, the premature end of the Lakanal House Working Group ensured that its failure properly to oversee the progress and completion of the steps that it had itself identified as necessary went unremedied.
The Lakanal House fire demonstrated, if not for the first time then beyond any lingering doubt, that combustible facade panels could enable fire to spread through the external wall of a high-rise building and that a failure of effective compartmentation, whether resulting from combustible facade panels or otherwise, could lead to the rapid total failure of a building. Understanding those risks, which were later to be exemplified in the Grenfell Tower fire, was essential, given the increasing prevalence of modern materials and methods of construction. We have therefore considered it appropriate to examine the extent to which the LFB understood the significance of the Lakanal House fire and how it affected its understanding of the hazards posed by combustible facade panels.
By December 2009, the LFB was aware that other buildings in London might be constructed of materials that would allow fire to spread rapidly across the external walls and result in a consequent widespread failure of compartmentation. Indeed, the exchange between Commissioner Dobson and Sir Ken Knight during December 2009 was prompted by the LFB’s belief that the regulatory regime was inadequate or was being widely ignored.[370]
When Commissioner Dobson was asked why the LFB had not taken steps at the time to advise its operational crews how to respond to the spread of fire across the external wall of a building, he said that he did not think that the way in which the fire had spread at Lakanal House had been unusual and that firefighters would not have been surprised to see the fire spread in the way it did, although they might have been surprised by the speed at which it had happened. He did not think there had been anything particularly unusual about the Lakanal House fire that crews needed to be notified of.[371]
We do not agree with the Commissioner’s assessment. Other witnesses told us that the spread of fire downwards at Lakanal House had been unusual. For example, Dr David Crowder described it as very unusual and not something that had been encountered commonly, if at all, previously.[372] Sir Ken Knight said that it had been almost unique.[373] Furthermore, it is clear that the crews at Lakanal House were surprised by both the speed and the direction in which the fire had spread.[374] Given that the LFB knew about the use of combustible panels in external walls and the risks associated with them, crews should have been expressly warned about the danger of fire spreading across them and the consequent risk of compartmentation failure.
National operational guidance on firefighting in high-rise buildings is to be found in Generic Risk Assessment (GRA) 3.2 issued by the DCLG. The version of GRA 3.2 in force at the time of the Lakanal House fire, published in September 2008, had identified the failure of compartmentation and the potential need for multiple rescues as an event for which contingency plans ought to be developed.[375] At the Lakanal House inquests, however, Commissioner Dobson told the coroner that under normal circumstances operational firefighters would expect a fire in a high-rise residential building to remain within the compartment of origin and not to enter communal areas before crews could reach the compartment and attack the fire.[376] He said that crews would have been aware that the fire might spread to flats immediately above the fire flat, but would not expect it to spread to flats that were adjacent to the flat of origin.[377] Peter Holland, who was the Chief Fire and Rescue Adviser at the time of the Lakanal House inquests, told the coroner that, although the compartmentation of a building was sometimes not as good as it was designed to be, a failure of compartmentation was an infrequent rather than a regular occurrence.[378]
On 9 July 2009, six days after the Lakanal House fire, Commissioner Dobson sent a letter to the housing departments of all London boroughs, housing associations and other social housing providers referring them to AC Turek’s letter of 23 March 2009.[379] In his letter he reminded recipients about certain fire safety matters, including the need for a suitable and sufficient risk assessment, which the letter said should include consideration of compartmentation, particularly where it protected escape routes. He also reminded them that a risk assessment should be reviewed if any material change was made to the premises, including any changes to the compartmentation arrangements or refurbishment.
In that letter the Commissioner drew attention to the need to have an evacuation strategy appropriate to the circumstances of the individual premises, but he emphasised that it should be safe for residents to remain in their flats if a fire occurred elsewhere in the building, providing that the premises complied with both the Building Regulations and the Fire Safety Order and suitable management and maintenance procedures were in place.
Commissioner Dobson agreed that when that letter had been written the early indication from the LFB’s own investigations had been that a failure of compartmentation had been one of the primary reasons for the spread of fire at Lakanal House and that he had been concerned that other buildings in London might suffer from the same defect.[380] However, he said that the reference to strategies for evacuating buildings had not been intended to suggest that a “stay put” strategy might not be appropriate for such buildings; rather, it had been prompted by the LFB’s understanding that the escape balconies at Lakanal House had not been used by residents because they had not been aware of their purpose.[381]
The widespread failure of compartmentation at Lakanal House was also identified in the action plan drawn up by the Lakanal House Board. Item 20 required the LFB’s Fire Safety department to carry out a review of high-rise fires involving the spread of fire beyond the compartment of origin to identify those incidents which could have provided opportunities for learning before 3 July 2009.[382] DC Dexter said that that had been a response to both the spread of fire that had occurred at Lakanal House and to emerging findings reported by the Fire Safety team.[383] Given the contents of AC Turek’s letter, it is surprising that a search of the LFB’s incident management system had not revealed any record of a high-rise incident at which fire had spread by mechanisms similar to those identified at Lakanal House.[384] DC Dexter later questioned that finding with the LFB’s Information Management department, which was responsible for collating and managing data of that nature.[385] In response, Clive Eustice, a member of the department, expressed doubt about the absence of any such records, which he thought reflected a very lazy response. Mr Eustice said that on being given the relevant criteria the department could provide a report setting out the relevant incidents, but no such report was made available to us.
When she was asked why she had raised the matter with the Information Management department, DC Dexter said that, having read a number of fire investigation reports, she could see that there had been breaches of compartmentation or the spread of fire beyond the compartment of origin and thought it unlikely that no incidents of that kind could be identified.[386] There is evidence that she did in fact obtain some data as a result of her inquiries and that she questioned whether Item 20 had been clearly defined.[387] Ultimately, however, the LFB concluded that there was no record of a high-rise incident at which fire had spread in ways similar to those at Lakanal House.
The conclusion that there had been no similar incidents before the Lakanal House fire was inconsistent with AC Turek’s letter of 23 March 2009. It was also inconsistent with concerns that were being discussed both within the LFB itself and by the LFB with outside bodies soon after the Lakanal House fire. On or around 21 April 2010, there was a meeting at the LFB’s headquarters between Commissioner Dobson and representatives of the construction industry, local authority building control, and representatives of the DCLG, including Brian Martin. AC Turek wrote a briefing note for the Commissioner in advance of the meeting which said that its purpose was to discuss the LFB’s concerns about the quality of construction and checking of newly built and newly refurbished residential properties.[388] Those concerns resulted from a significant number of fires during the previous two years which had exhibited an unusual spread of smoke or fire. The note stated that the causes had often been identified as breaches of the Building Regulations, either during construction or refurbishment, and that the fires had led to people becoming trapped and requiring rescue, the collapse or other unnecessary damage to buildings and to firefighters’ being placed at unnecessary risk. There had been about 50 significant cases in the London area, most of which were said to have involved major construction companies. The note referred to the concern felt within the LFB about whether the regulations covering the construction and approval of building work were being enforced with sufficient vigour to ensure that new residential buildings in London were fit for their purpose, as well as to concern about how many such buildings there might be in the city.
The briefing note did not provide details of any of those significant cases in London, but other evidence suggests that the fire at Bush House on 2 February 2007 had prompted the meeting. Bush House was a six-storey, newly constructed residential block. A fire had started in the basement parking area and entered a service shaft, through which it spread vertically to all floors of the building, including the building’s only escape route, resulting in residents having to be rescued by the fire brigade from the balconies of their flats.[389] As a result of the concerns raised by that and other similar incidents, those present at the meeting agreed that the National House Building Council (NHBC), in conjunction with the Chief Fire Officers Association, would provide training to raise awareness of the need for effective fire stopping. That training was provided in 2011.[390]
Commissioner Dobson was unable to recall any details of the meeting, but he agreed that by April 2010 the LFB had identified the risk across the built environment of failure to comply with the Building Regulations and was aware that it had resulted in a significant number of fires in London.[391] He told us that the way in which the fire had spread at those incidents had been predictable, given the defects in the buildings,[392] and he agreed with DC Dexter that the failure of compartmentation was common, although for a wide range of reasons.[393] Nonetheless, the LFB did not seek to communicate the existence of those defects or their concerns about defective buildings to operational crews. Commissioner Dobson said that he had had concerns about the proliferation of guidance and information given to operational crews, because complaints had been made in the past that guidance notes often duplicated or conflicted with one another.[394] Mr Dobson also told us that in any event, the spread of fire as a result of inadequate compartmentation would generally not be a surprise to operational firefighters.[395]
Although the Commissioner’s concern not to over burden operational crews with excessive guidance was understandable, we think it would have been possible to communicate to crews in a simple way that the LFB was coming across a significant number of buildings that did not comply with the Building Regulations and that crews therefore needed to be ready for smoke and fire to spread in unusual ways as a result of a failure of compartmentation. That would have sent a clear message that was consistent with national guidance and, more importantly, would have reflected the dangers that the LFB was encountering on the ground. If there was an unhelpfully large amount of operational guidance in circulation, the LFB should have taken steps to reduce it, but that was not a good enough reason not to draw the attention of operational personnel to concerns about inadequate compartmentation that were very much in the minds of those at senior management level.
Inadequate compartmentation in residential high-rise buildings continued to be a concern to the LFB throughout its investigations into the Lakanal House fire. On 11 December 2012, Commissioner Dobson wrote to Brandon Lewis MP, then Parliamentary Under-Secretary of State with responsibility for fire and resilience,[396] setting out seven recommendations that the LFB thought should be considered by the government. The first was that the government should provide further guidance on which parts and areas of buildings containing multiple domestic premises could be described as ‘parts used in common’ for the purposes of the Fire Safety Order and how that order was intended to operate in relation to premises where the responsible person did not necessarily have control over features affecting the common parts or common fire precautions. Commissioner Dobson said that the recommendation had been identified by the LFB following the failure of compartmentation that had occurred at Lakanal House and, in particular, the fact that the fire had spread from the flat of origin into the adjacent corridor much faster than it would have expected.[397] We consider the other recommendations in the letter elsewhere.[398]
In her rule 43 recommendations the coroner at the Lakanal House inquests also identified a failure of compartmentation as a matter that required greater consideration by both the LFB and DCLG. In her letter to the LFB, she recommended that consideration be given to the training of incident commanders and potential incident commanders to enhance their performance in seven specific respects, including the ability to recognise that a fire might behave in a manner inconsistent with the principle of compartmentation.[399] The LFB’s response to that recommendation is considered below. In her letter to DCLG, the coroner recommended that consideration be given to reviewing GRA 3.2 to provide consolidated national guidance on four particular matters, including awareness that insecure compartmentation can permit the transfer of smoke and fire between a flat or maisonette and common parts of high-rise residential buildings, which has the potential to put the lives of residents and others at risk.[400] In the event, the LFB effectively took charge of the review of GRA 3.2 following the Lakanal House fire.
It is clear from her rule 43 letter that the coroner considered that operational crews, and incident commanders in particular, needed to be prepared for the risk that compartmentation within a high-rise residential building might fail, even though Commissioner Dobson had told her that in his view it remained appropriate to base plans for firefighting and rescue operations on the assumption that compartmentation would be effective. The coroner did not find that the LFB should have reversed the “stay put” advice to residents or that it should have evacuated the building, but in the DCLG’s response to the rule 43 letter sent to the coroner on 20 May 2013 by the Rt. Hon. Eric Pickles MP, Secretary of State for Communities and Local Government, there was explicit recognition of the possibility that “stay put” might no longer be a tenable strategy if there were a failure of compartmentation. Referring to the pending review of GRA 3.2, the letter confirmed that the revised guidance would include advice to incident commanders to inform decisions on evacuation, should it become clear during an incident that the “stay put” principle was no longer tenable.[401]
In contrast, it appears that no-one within the LFB gave any serious thought to the potential limitations of the “stay put” strategy either before or after the Lakanal House fire, notwithstanding the concerns expressed within the organisation about inadequate compartmentation and the rapid spread of smoke and fire that had occurred at Lakanal House. AC Daly, the head of the Fire Safety department at the time of the Grenfell Tower fire, rightly acknowledged that the “stay put” strategy is absolutely dependent on effective compartmentation.[402] The LFB’s own documents, even those which pre-dated the Lakanal House fire, such as AC Turek’s letter of 23 March 2009, referred to breaches of compartmentation that were significant and posed a real threat to residents’ safety. Those concerns should have prompted an analysis by the LFB of the circumstances in which a “stay put” strategy would need to be kept under review, and potentially abandoned, during the course of an incident.
It is not clear why the LFB failed to undertake such an analysis following the Lakanal House fire. On the one hand, there was sufficient concern within the organisation about inadequate compartmentation for it to call a meeting with government and industry in April 2010; on the other, senior officers appear to have assumed that operational personnel were accustomed to dealing with failures of compartmentation when they occurred. Consequently, no serious thought was given to sharing with station-based crews the concern of senior officers about the prevalence of inadequate compartmentation in London or the potentially very serious consequences that could follow if compartmentation were to fail.
In the light of the Lakanal House inquests it became clear to the LFB that there was a need to provide additional training to firefighters and more senior officers in responding to events of the kind that had occurred at that fire. A training package was therefore produced known as the Lakanal House Case Study.[403] It was commissioned in June 2013, but staff did not start to receive training until July or August 2014, over a year later and five years after the fire.[404] The case study consisted of a computer-based training package for station-based staff and a half-day presentation for those of station manager rank and above.[405]
In 2018 the LFB produced a report for the Inquiry containing a review of the action it had taken in response to the Lakanal House fire.[406] Both that report and several LFB witnesses[407] suggested that a wide range of measures that had been taken in response to the fire had been covered in the case study, but that was not correct, because it dealt with only a relatively narrow range of operational topics, in particular:
The case study did not provide any or adequate training in the following important operational matters in respect of which the Lakanal House fire had exposed weaknesses:
Director Reason said that the risk of a failure of compartmentation had been implicit in the training,[408] that the whole package had been concerned with recognising when compartmentation had failed,[409] and that the graphics and all the material used in the package had been self-evident[410] or otherwise should have been obvious to firefighters.[411] However, the contents of the package do not, in our view, bear that out. They did not make it clear that compartmentation could not always be relied on and did not provide guidance on how to identify or deal with a failure of compartmentation. Those omissions, together with the emphasis on the Lakanal House fire being highly unusual, tended to perpetuate the assumption that compartmentation in high-rise buildings could be relied on.
The omission of any reference in the package to the dangers arising from the use of combustible panels in external walls is particularly surprising in view of the fact that Commissioner Dobson had written to the government in December 2009 expressing the LFB’s concern about compliance with the Building Regulations in general and the particular risks posed by certain kinds of external cladding. By that time the LFB had discovered that other buildings in London might be constructed from materials that could result in the rapid or unusual spread of fire across or through external walls.
The present Commissioner, Andrew Roe, suggested that the case study was more sophisticated than might appear from the slides that had been put to certain LFB witnesses. He pointed out that the computer-based package had been accompanied by a training guide and that use had been made of the radio messages sent during the incident as well as interviews with principal officers who had attended the fire.[412] Although they may have made the training more engaging and provided an insight into the attending officers’ experience, they did not make up for the omissions identified above.
Commissioner Roe rightly accepted that the case study should have dealt with the failure of compartmentation on a widespread scale and the danger of external fire spread, both of which had played a critical part in the Lakanal House fire. He accepted that knowledge held by one part of the organisation should have been shared widely and included as part of the package.[413]
Director Reason said that the training package had been seen by the Commissioner, Deputy Commissioner and the Directors and that, to his recollection, no concerns had been raised about its general content or whether it covered the coroner’s recommendations effectively.[414] The training package was not subsequently reviewed to ensure that it dealt with them adequately,[415] other than by identifying any deficiencies in operational responses identified through routine IMP database reports submitted to the co-ordination board.[416]
Although a number of senior LFB witnesses regarded the case study as a key element of its response to the Lakanal House fire,[417] it fell far short of what was required. The delay of five years between the fire and the release of the training package emphasises the LFB’s failure to identify quickly the important lessons to be learnt from the incident and provide the necessary training as quickly as possible. That failure was compounded by the fact that the training package failed to address the most important aspects of the Lakanal House fire. It was primarily a narrative account of the incident, which limited its value as training for crews. Director Reason said that the package had not been intended for use in isolation, but together with other training packages, although he accepted that it was necessary for officers themselves to find the relevant packages or policies to study.[418] Given the nature and potential scale of the dangers revealed by the Lakanal House fire, it was not appropriate to rely on individual officers to take the initiative to that extent. The situation was further worsened by the failure of other LFB training programmes to cover all the coroner’s recommendations.
The LFB’s knowledge about the risks posed by combustible panels should have been communicated to operational crews through appropriate additions to the training programme in late 2013 after it had become clear from correspondence with DCLG about the meaning of functional requirement B4(1) that the government would not take any steps (at least in the short term) to address the problem. Regrettably, however, that did not happen. There were no relevant changes in training and the information was not adequately communicated to operational crews. When asked about the failure to inform crews about these risks, Commissioner Dobson said they were matters that concerned the Fire Safety and Enforcement arms of the LFB, rather than the operational crews.[419] That view was both wrong and short-sighted. Although compliance with the Building Regulations was no doubt a primary concern of the Fire Safety and Enforcement departments, the consequences of an extensive failure of compartmentation resulting from the use of combustible materials which allowed fire to spread rapidly across the external wall of a building would directly affect operational crews. They had particular implications for incident commanders implementing a “stay put” strategy that was still regarded within the LFB as underpinning the approach to fighting fires in high-rise buildings at the time of the Grenfell Tower fire.
The Lakanal House fire should have alerted the LFB to the possibility that ineffective compartmentation throughout a high-rise residential block might result in a rapid total failure of the building. LFB witnesses maintained in their evidence to us that the risk of a failure of compartmentation was an important lesson taken from the Lakanal House fire and referred to training initiatives subsequently introduced, including the case study, as having enhanced operational crews’ understanding of that risk and how to respond to it.[420] However, that was far from the case. In fact, the important subject of how to identify and respond to a failure of compartmentation remained strikingly absent from LFB training and policy following the Lakanal House fire. It was not mentioned in the revised edition of GRA 3.2 published in 2014, which the LFB was largely responsible for drafting, or in the incident command training that the LFB introduced in response to the coroner’s recommendation.
The LFB’s response to the Lakanal House fire placed undue reliance on process. Plans were made, boards were established and reviews were commissioned, but the process failed to ensure that the organisation fully understood and acted on the different aspects of its experience at the Lakanal House fire, in particular the danger of relying on compartmentation, the risk of fire spreading across external walls and the importance of being able to handle many fire survival guidance calls simultaneously. The LFB’s failure to understand the importance of those matters is illustrated by their omission from the training package. The truth is that the LFB failed to consider in a systematic and rigorous way whether the outcome of the process provided an effective response to the questions raised by the fire.
By the summer of 2016, the Lakanal House fire was not the only source of information available to the LFB about the risk of rapid external fire spread and the consequent loss of compartmentation associated with the use of modern building materials and the problems to which that can give rise. In this chapter, we consider other sources of information about the dangers posed by the use of combustible materials in external walls and the experience of the LFB at other fires in high-rise buildings in London.
First, we consider a fire that occurred in a building called Madingley in Kingston-on-Thames in July 2010 and certain correspondence between the LFB and DCLG about the effect of functional requirement B4 that took place between February 2011 and October 2013. We then consider in this context fires in high-rise buildings abroad, to which we referred in Chapter 11. Finally, we consider two fires that broke out in high-rise residential buildings in London, Adair Tower in October 2015 and Shepherd’s Court in August 2016. Both incidents illustrated the LFB’s practical approach, following the Lakanal House fire, to the risks posed by combustible cladding (in particular, the prospect of a complete failure of compartmentation), the need to evacuate parts of a high-rise building and how best to carry out an evacuation.
Not long after Commissioner Dobson’s exchange of correspondence with DCLG at the end of 2009, another incident occurred in London involving the spread of fire through combustible materials in a building’s façade. The fire at Madingley, a 17-storey residential building in Kingston-upon-Thames, occurred on 12 July 2010. It started in a flat on floor 12, spread rapidly through a plastic rainwater pipe system to flats on floors 13, 14 and 15 and thence to the roof of the building. Smoke entered the building’s escape stairs on floor 15. Twenty fire appliances attended the incident. About 80 people evacuated the building; no-one was injured.[421]
Tests carried out by both Bureau Veritas and the LFB established that the rainwater pipe system was the principal means by which the fire had spread, but other materials forming part of the balconies and the edge of the roof were also examined. It was found that glass-reinforced plastic fascia panels and polystyrene insulation on the balconies were easily ignited and, once ignited, continued to burn and spread flames rapidly, producing large amounts of black smoke. A castellated roof fascia panel was found to behave in the same way. Bureau Veritas concluded that those elements could contribute significantly to the overall intensity of a fire and its combustion products.[422]
Messages passing between some of those in the LFB who were investigating the Madingley fire show that they considered the possibility that the other three blocks on the estate could contain similar materials and discussed whether it would be appropriate to implement an “early evacuation” strategy rather than “defend in place” if there were another fire.[423] The evidence we have seen, however, suggests that the change was not made and that crews were not given any warning about those risks.[424]
Between February 2011 and October 2013, the LFB entered into correspondence with DCLG in an attempt to obtain clarification of the effect of functional requirement B4(1) (the requirement that the external walls of a building shall adequately resist the spread of fire over the walls and from one building to another, having regard to the height, use and position of the building). Following the receipt of advice from a retired building surveyor, the Commissioner had become concerned that the language used did not make it clear that the ability adequately to resist the spread of fire over external walls was a requirement in its own right. Indeed, the person from whom the Commissioner had taken advice thought it was not. As the LFB recognised at the time, that was an incorrect interpretation, but it suggested that there might be widespread misunderstanding about the effect of functional requirement B4(1) that was shared even by some building control officers. That was potentially a matter of national importance.
The attempt to obtain a definitive interpretation of the regulations failed because DCLG was unwilling to provide formal clarification of the effect of functional requirement B4(1), but the correspondence clearly shows that senior officers in the LFB were aware that there was considerable uncertainty in the construction industry about its meaning and that there was a potentially widespread failure to comply with the requirements of the Building Regulations in relation to the external walls of high-rise buildings. They expected the problems to increase in the absence of effective regulatory intervention.[425] The LFB did all it reasonably could to persuade the government that action was required, but its concerns were not properly addressed. Nonetheless, the episode had served to draw the attention of the LFB to the uncertainty in the construction industry surrounding the meaning of functional requirement B4(1), and provided it with an opportunity to consider what, if any, changes were required to existing training, operational policies and procedures.
The LFB’s knowledge of the risks posed by combustible panels should have been communicated to operational crews through appropriate additions to the training programme in late 2013 after it had become clear that the government would not take any steps (at least in the short term) to address the problems identified in the correspondence. Regrettably, however, that did not happen. There were no relevant changes in training and the information was not adequately communicated to operational crews. When asked about the failure to inform crews about those risks, Commissioner Dobson said that they were matters that concerned the Fire Safety and Enforcement arms of the LFB, rather than the operational crews.[426] That view was both wrong and short-sighted. Although compliance with the Building Regulations was no doubt a primary concern of the Fire Safety and Enforcement departments, the consequences of an extensive failure of compartmentation resulting from the use of combustible materials which allowed fire to spread rapidly across the external wall of a building would directly affect operational crews. They had particular implications for incident commanders following a “stay put” strategy, which was still regarded within the LFB as underpinning the approach to fighting fires in high-rise residential buildings.
In Chapter 11 we have referred to the information available about fires in high-rise buildings in other countries, all of which involved to a greater or lesser degree the spread of fire across external walls. Before the Grenfell Tower fire occurred, the LFB had no system for recording fires of that kind, for investigating why or how they had occurred, or for considering whether they contained any lessons for fire prevention or high-rise firefighting in London. The main reason for that omission appears to have been a widely-held assumption that fires of that kind could not occur in this country because the Building Regulations did not allow buildings to be constructed in a way that would allow the spread of fire over the external walls. There was also a prevalent view that the UK’s regulatory regime was superior to, and more robust than, those in other countries.[427] Two examples demonstrate the shortcomings of this approach to the gathering and analysis of information from fires outside this country.
The Lacrosse fire caused the authorities to carry out an audit of Melbourne’s high-rise buildings. In March 2016, the LFB was provided with the results of that audit, which revealed that 51% of the buildings surveyed did not comply with the regulations. AC Daly was asked whether that ought to have alerted the LFB to the possibility that the position in London might be similar. It was a relevant question, because, as we have pointed out, the LFB’s reliance on the existence of a robust regulatory system in the UK necessarily depended on compliance with it. His response was that it was likely that the question had been raised within the LFB at the time, but that there was no evidence that there were buildings in London that used external wall cladding that did not comply with the Building Regulations.[428] The explanation was unsatisfactory, first, because there is no evidence that the question had actually been considered in that way, and secondly, because the purpose of any investigation would have been to discover whether there had been a widespread failure to comply with the regulatory requirements. In our view, the unexpectedly high rate of non-compliance found in Melbourne was a compelling reason for the LFB to consider whether the same problem existed in London.
Information about the fire at the Address building in Dubai reached senior officers of the LFB through DAC Graham Ellis who sent an email to two of his LFB colleagues containing a link to an article about flammable polyurethane and aluminium cladding involved in a fire in Dubai.[429] He copied his message to AC Cotton in her capacity as Head of Operational Assurance. The article said that the fire had resurrected fears about the widespread use of highly combustible materials on skyscrapers across the UAE. It also said that a fire safety expert had estimated that up to 70% of Dubai’s high-rise buildings could be clad in polyurethane and aluminium composite cladding, notwithstanding the requirement in the UAE that buildings over 30 metres in height be constructed from non-combustible materials. Towards the end of the article the author referred to the regulatory position in Britain, which he said did not permit any surface spread of flame.[430]
Responding to the email from DAC Ellis, GM Biles made a flippant comment about paragraph 12.7 of Approved Document B, which provided by way of guidance that insulation products and filler materials should be of limited combustibility. AC Cotton replied to his comment, also in flippant terms. Neither paragraph 12.7 nor the broader requirements of Approved Document B had been mentioned in the body of the article, but they had been mentioned in a comment made by an online user who drew attention to the distinction between a Class 0 surface and a combustible core and asserted that there were large schemes still being constructed in the UK for which similar panels were being incorrectly specified due to a fundamental misunderstanding of the regulations.
AC Cotton said that she had not read the comments below the main body of the article,[431] but the reference to clause 12.7 in his comment shows that, at the very least, GM Biles had. We think it surprising that none of those who received the email thought it necessary to draw the attention of the Fire Safety department to the article or the online comment, given that the comment suggested that there was a fundamental misunderstanding within the construction industry about the requirements of the Building Regulations relating to materials used in external walls. The exchange also revealed a failure by senior officers adequately to probe and question information they did not fully understand. Most importantly, the LFB should have been alert to the risk that there might be many buildings in London with dangerous cladding, but it was too complacent to discover the existence and extent of any problem in London before it was too late.
On 7 July 2016 members of the LFB’s Fire Safety department attended a seminar organised by the NHBC entitled “Facades to Tall Buildings”. One presentation contained images of fires in high-rise buildings both in the UK and abroad, including the Address Tower fire in 2015 and the Tamweel Tower fire in 2012, both in Dubai, and the Garnock Court fire in Glasgow in 1999.[432] It also contained diagrams depicting different mechanisms of external flame spread taken from BR135 Fire performance of external thermal insulation for walls of multi-storey buildings (3rd ed., 2013) and relevant extracts from Approved Document B and Building Control Alliance Technical Guidance Note 18.[433] The content of the seminar was subsequently used to create the LFB’s own presentation entitled “Tall Buildings Facades”.
AC Daly said that the conference had been seen as providing reassurance about conditions and regulations in this country.[434] However, we draw exactly the opposite conclusion. First, in the course of the seminar the NHBC warned about the dangers of highly combustible polythene-cored ACM products, the omission of cavity barriers around openings, unrealistic assumptions about the fire resistance of glazing and confusion between the fire resistance of a wall assembly and fire spread across or within it.[435] Secondly, the Building Control Alliance, in a presentation on demonstrating compliance with the Building Regulations, had separately sounded a warning about a number of matters, including the absence of any tests using lightweight metal claddings, desktop assessments by fire engineers being based on opinion rather than fact, and the substitution of materials.[436] Thirdly, Brian Martin’s presentation on regulatory requirements contained a diagram taken from BR135 which showed how combustible cladding systems could contribute to the spread of flame and the risk of secondary fires.[437] Fourthly, the BRE explained the mechanisms of external fire spread involving combustible materials and stated that the BS 8414 test method was being used in the same or a substantially similar way in the UAE, Australia and China.[438]
The LFB was well aware of those warnings. It should, therefore, have been aware of the importance of understanding the risk of rapid external fire spread in buildings in London. The LFB’s own “Tall Buildings Facades” presentation[439] carried a number of relevant warnings. First, it warned that although it was a general principle that the external envelope of a building should not contribute to the spread of fire, new construction materials and methods of construction were being used in facades with a limited understanding of their behaviour when exposed to fire. The same slide warned that such materials could affect the way that fires develop and spread in a building. Secondly, it warned of the importance of the facade’s not contributing significantly to the spread of fire. Thirdly, it identified combustible materials in the facade as likely to lead to the spread of fire. Fourthly, it reproduced the diagrams in BR135 depicting the mechanisms of external fire spread. Finally, it concluded that the construction of the facade of Shepherd’s Court might have contributed to the fire spread. There was, therefore, nothing in the various presentations to justify an unqualified assumption that the risk of rapid external fire spread was, in some way, restricted to methods of construction used abroad.
The evidence from fires abroad and the warnings and concerns expressed about building methods used in this country partly reflected, but certainly confirmed, the LFB’s knowledge of, and longstanding anxiety about, a widespread failure to comply with the Building Regulations in London and, in particular, about modern construction materials which caused or permitted the unusual spread of smoke and fire. That knowledge and those worries pre-dated the Lakanal House fire in July 2009 and were reinforced by the Shepherd’s Court fire in August 2016, discussed below.
Commissioner Cotton said she was unaware that anyone in the LFB had ever brought the risk of failure to comply with the Building Regulations to the attention of senior officers.[440] She told us that neither she nor the Operational Assurance department had been made aware that the LFB knew about problems caused by poor compartmentation (and the implications for a “stay put” strategy) until April 2017, when a letter raising the question had been drafted by the LFB’s Fire Safety department and sent in her name (as Commissioner) to Gavin Barwell MP and Brandon Lewis MP (Minister for Housing and Minister for Policing and the Fire Service respectively).[441] She said that the Operational Assurance department had never been asked to consider the risks resulting from failure to comply with the Building Regulations or the spread of fire resulting from an inappropriate choice of materials, which had never been brought to its attention.[442]
It is clear to us that communications between the different departments of the LFB were very limited and that as a result there was a significant failure to ensure that important information, in this case information about threats to the built environment, was shared with departments which really needed to receive it. The Fire Safety department should have worked much more closely with the Operational Assurance department to investigate significant fires in other countries and to understand whether there was anything important to be learnt from them. Instead, there is no evidence that either of those departments, or indeed any other department, used them as a means of improving their understanding of the risks associated with modern and refurbished buildings and their ability to fight fires in high-rise buildings. That reflected both a failure of organisation and management and a failure on the part of individual officers to display the breadth of vision to be expected of them.
Two other fires in high-rise residential buildings occurred in London following the Lakanal House fire, both of which gave rise to challenges similar to those that had been encountered at that fire and were to be encountered again at the Grenfell Tower fire. The first was the fire at Adair Tower; the second was the fire at Shepherd’s Court.
Adair Tower is a 14-floor residential building. On 31 October 2015, a fire was started by a lighted firework being put through the letterbox of a flat on the third floor. When the first crews arrived, they reported a fully developed fire that had spread into the adjoining lobby. Neighbouring flats were affected by smoke and heat, as were the main stairwell and communal lobbies on higher floors. There were no self-closing devices on the doors of the flats, which made it easier for smoke to spread. 19 pump appliances attended the fire.[443]
A considerable number of calls were made by residents of Adair Tower to the control room during the course of the incident, including calls during which fire survival guidance was given. The LFB’s records were not consistent in recording the number of fire survival guidance calls.[444] Up to six fire survival guidance calls (depending on how they were characterised) were received between 08.54 and 09.08, together with 15 other calls.[445] In any event, the total number of fire survival guidance calls made during the Adair Tower fire exceeded the five received during the Lakanal House fire.[446] The incident commander, GM Anthony Biles, who had 34 years of operational experience, said that it was the highest number of fire survival guidance calls that he had dealt with in his career.[447] Fifty residents were helped to escape the building, either by firefighters or by control room officers (CROs) who provided advice and guidance.[448]
When GM Biles arrived at the incident ground, he realised that many people were trapped and needed to be rescued, or believed that they did, so he obtained additional crews with extended duration breathing apparatus (EDBA) to conduct search and rescue operations on higher floors and hand over residents they had rescued to firefighters wearing standard breathing apparatus on the lower floors. GM Biles did not formally revoke the “stay put” strategy, but he briefed crews to clear the building.[449]
The incident monitoring process report recorded that there had been good handling of a large volume of fire survival guidance information with finite resources. There was no reference to the evacuation of residents or the “stay put” strategy.[450]
Shepherd’s Court is a 20-floor residential building in Shepherd’s Bush. On 19 August 2016, a fire started in a faulty appliance in a flat on floor 7. It spread to floors 8, 9, 10 and 11 through external facade panels and entered some of the flats on those floors through open windows. The block’s single stairwell had a good level of compartmentation and individual flats had good fire doors with self-closing devices. Twenty appliances attended the fire, which was ultimately extinguished.[451]
SM Charles Hanks was the second incident commander, having assumed command about 34 minutes after the first crews had arrived.[452] He remained in command for about ten minutes until GM Richard Ogden arrived.[453] During that ten-minute period he saw that the fire had spread to the floor above the flat of origin, which he recognised indicated a possible failure of compartmentation. Soon after, SM Hanks was told that a third floor had become involved in the fire. He became concerned that there was a risk that the fire might spread further externally and also a risk that it might spread in the interior of the building.[454] He described the spread of fire as “exceptional”, although there had been very little spread of smoke and flame in the interior and the stairwell had not been affected.[455]
Once SM Hanks had become aware that three floors had become involved in the fire, he decided that he needed to ensure that the flats immediately above the fire were empty and that any occupants were moved to safety when possible. (He said that, if necessary, he would have carried out a controlled evacuation of the occupants from the flats on the 9 floors immediately above because the fire was spreading vertically but not sideways.) At the same time, he directed crews to begin a systematic search from the top of the building, moving downwards to obtain information about the conditions within the building rather than to carry out search and rescue operations or to evacuate flats on those higher floors. His strategy was not intended to undermine the “stay put” policy, which in his view was maintained throughout, but was in his view a sensible precaution for one or two flats when conditions allowed, given that fires can occasionally jump a compartment boundary.[456] The LFB’s Fire Investigation report records that approximately 50 people had been evacuated from the building.[457]
The LFB has rightly accepted that, before the Grenfell Tower fire, it had failed to train its incident commanders to understand when and how to carry out an evacuation of a high-rise residential building with a “stay put” strategy in the absence of an existing plan.[458] It was a failing which had the most serious consequences for the residents of Grenfell Tower on the night of 14 June 2017.[459]
It must also be acknowledged, however, that the LFB was not alone in this failing. At the time of the Grenfell Tower fire there was no national operational guidance on how to evacuate a residential high-rise building[460] and it does not appear that any other fire and rescue service in the United Kingdom had included in their operational policies or training any guidance on the practical aspects of carrying out an evacuation, beyond saying that it should be considered, as in PN63. On that basis, we agree with DAC Cowup’s description of evacuation as a blind spot for the LFB. There is also some evidence to suggest that it may be a blind spot for other fire and rescue services, although we have not heard evidence about current firefighting practice outside London and Kent.[461]
Nonetheless, the operational responses to the Adair Tower and Shepherd’s Court fires demonstrate that, although the LFB was not training its commanders on the evacuation of high-rise residential buildings, nor providing for it in its policies, it contained officers who were capable of carrying out some form of successful evacuations in high-rise residential buildings and, when circumstances required, did so. Commissioner Roe referred to incidents within his own knowledge where there had been a partial failure of compartmentation and where the incident commander had made a decision to evacuate the floors above and below the fire, while the rest of the residents remained in their flats. Commissioner Dobson also agreed that evacuation was not an unusual occurrence and that firefighters were well acquainted with evacuating all sorts of buildings, including high-rise buildings.[462] DAC Cowup similarly told us that evacuation was a fairly routine and intuitive process, though he accepted that before the Grenfell Tower fire the LFB had not understood the need to provide firefighters with specific guidance on it.[463]
It is important to note that evacuation is not necessarily inconsistent with a “stay put” strategy. If residents are being adversely affected by heat, fire or smoke, their evacuation is entirely consistent with such a strategy. However, the evacuation of flats which are not adversely affected by heat, fire or smoke does involve a revocation, at least in part, of a “stay put” strategy. There was no reference to the “stay put” strategy or to the partial evacuation of residents in the IMP reports on either the Adair Tower or the Shepherd’s Court fires,[464] but we are satisfied that in practice some incident commanders have carried out emergency evacuations, including the evacuation of flats not adversely affected by smoke or fire, of some kinds of residential high-rise buildings with “stay put” strategies without recording the fact. It is not possible to say with confidence how frequently they have done so, but Adair Tower and Shepherd’s Court do not appear to have been isolated incidents. The incident commanders at both fires appear to have acted intuitively, without notifying the control room, and no one appears to have regarded their actions as particularly significant. That suggests that the approach taken at both those incidents was not out of the ordinary. Indeed, Commissioner Roe referred to incidents within his own knowledge where there had been a partial failure of compartmentation and where the incident commander had made a decision to evacuate the floors above and below the fire, while the rest of the residents remained in their flats.[465]
The evidence suggests that before the Grenfell Tower fire evacuations of high-rise residential buildings had been partial rather than total.[466] (At any rate, we have not been provided with any evidence of a total evacuation of a residential high-rise building in London or elsewhere in the United Kingdom.) As was the case at Adair Tower and Shepherd’s Court, such evacuations were probably carried out without discussion with the control room and perhaps without the commander necessarily considering whether the “stay put” strategy had been revoked. In such instances, it was the individual commander who made the decision based on his or her own judgement, deploying such practical strategies for the implementation of the evacuation as he or she saw fit. Before the Grenfell Tower fire, it was, ultimately, a matter of chance whether the officer acting as incident commander at any given time had sufficient experience and confidence to evacuate a high-rise residential building, despite the absence of any training on when and how to do so.
None of this undermines the conclusion in the Phase 1 report that “stay put” had become an article of faith for the LFB.[467] Institutionally, it was indeed so and the response at Grenfell Tower reflected that fact. However, the evidence heard in Phase 2 identified an inconsistency of approach and whether the incident commander considered evacuation owed nothing to established policy.
Another aspect of the Shepherd’s Court fire that prefigured the hazards encountered at Grenfell Tower was the use of combustible facade panels, in that case containing polystyrene insulation. On his arrival at the incident AC Daly, who was the most senior incident commander to attend the fire, saw fire spreading over the walls, which he thought was unusual because he would not have expected exterior panels to support combustion.[468] He thought it was the same phenomenon as had been observed at the Lakanal House fire.[469] AC Daly consulted SM James Flin, who was in attendance as a fire safety officer and was also a fire engineer, and the two of them agreed that it was necessary to find out why the spandrel panels appeared to have spread the fire.[470]
On 29 August 2016, sample panels were duly sent to Bureau Veritas for testing which was witnessed by personnel from the Fire Engineering team in the LFB’s Fire Safety department.[471] The panels contained a blue polystyrene foam insulation mounted on a plywood board. One of the samples had a steel facing sheet; the steel sheet of the other had become detached during the fire, exposing the foam beneath. The sample panels were exposed to three flame tests. In the case of the panel without a steel facing sheet, the blue foam was rapidly destroyed, creating flaming droplets and sustaining burning even after the removal of the flame source. One of the tests had to be stopped due to concerns about the height of the flames. In its report of 30 November 2016 Bureau Veritas confirmed that the panels were likely to have assisted the fire in spreading up the outside of Shepherd’s Court.[472]
On receipt of those findings, Charles Elie-Romeyer, a fire engineer in the LFB’s Fire Safety department who had witnessed the tests, revised the “Tall Buildings Facades” presentation to reflect the Shepherd’s Court incident so that it could be used at a training day for senior fire safety officers.[473] In the section on the Shepherd’s Court fire added by Mr Elie-Romeyer, the results of the Bureau Veritas tests were set out, including photographs of the burning sample panels together with the observation that the facade might have contributed to the spread of fire.[474]
AC Daly confirmed that the presentation had not been shared with anyone outside the Fire Safety Department, and, in particular, that it had not been shared with operational crews because of what he described as the very technical nature of the information relating to quite a complex area which operational personnel could not be expected to grasp or understand.[475] The Commissioner accepted that the presentation reflected the Fire Safety department’s knowledge of the potential for modern construction materials to promote the rapid spread of fire, and that there had been a failure to ensure that that information was communicated to the rest of the LFB, including operational staff.[476]
The Fire Safety Department’s continuing concern about compartmentation had previously been reflected in a report by Ms Adreena Parkin-Coates entitled Compartmentation Issues within the Built Environment published on 26 November 2015. Ms Parkin-Coates was a qualified fire engineer and a business support manager in the Fire Safety Department.[477] Like the later Jack report of August 2016, the Parkin-Coates report referred to the importance of adequate compartmentation in defining a building’s evacuation strategy. It also asserted that instances of inadequate compartmentation were widespread. In her summary of the report Ms Parkin-Coates noted that the success of many evacuation strategies, particularly “stay put” strategies, depended on adequate compartmentation, but that fire safety officers were becoming increasingly aware of defects in fire-stopping in new and refurbished buildings. She concluded that defects in compartmentation were widespread due to poor workmanship or a lack of oversight by building control bodies and contractors and that an overall strategy to address them was needed.[478]
In her report Ms Parkin-Coates accepted a view expressed by others that there was an endemic problem of sub-standard fire-stopping.[479] AC Daly thought that the use of the word “endemic” was likely to reflect the frequency with which defects in compartmentation had been identified in the pool of buildings that had been found not to comply with the Building Regulations during fire safety audits conducted by the LFB. (He said that about 70% of premises were found to be broadly compliant.) He accepted, however, that within that smaller pool of buildings, defects in compartmentation were identified reasonably regularly. He did not agree that sub-standard compartmentation was endemic across the built environment as a whole.[480]
Ms Parkin-Coates also referred to the Bush House fire in 2007, which had prompted a meeting with the government and other interested parties in 2010, and to the NHBC training initiatives that had been implemented in association with the Chief Fire Officers Association in 2011.[481] She also referred to and annexed a separate report entitled Structural Fire Safety Failures – Quarterly/Annual Reporting dated March 2015, which was provided to the Performance Management Board with her report because it was said to identify a number of other fires at which structural defects had been found.[482] The quarterly report for the period April to December 2014 recorded that 25 fires had occurred, three of which had exhibited possible defects in structural fire safety features that might have contributed to the development of the fire. All three of those fires, which included the fire at Holcroft House, had occurred in residential blocks of flats.[483] As noted earlier, the report recorded that some of the structural defects affecting fire safety identified at those incidents ought to have been recorded on the relevant building’s ORD entry, but had not been.[484]
AC Daly told us that the Parkin-Coates report, with all its appended reports, had been waiting for his attention when he took over as Head of Fire Safety in March 2016.[485] He told us that the material had given him cause for concern and that it had indicated that there were systemic issues that needed to be addressed.[486] He accepted that his concerns suggested that there were things that operational firefighters as well as the Fire Safety department needed to learn and accepted that the LFB had not always gained as much from the work of the Fire Safety department as it could have, in particular by involving operational crews in its thinking.[487] It is notable that, in the revised version of the Parkin-Coates report prepared in December 2016 for presentation to the Corporate Management Board, the range of suggestions for action related to the Fire Safety department and Fire Safety personnel alone. There was no suggestion that operational personnel should be involved in any way in the measures proposed for remedying inadequate compartmentation.[488] We accept that it was not a deliberate omission,[489] but it is significant for what it tells us about the nature and extent of the collaboration between the fire safety and operational sides of the LFB.
In late 2016, at the time that the Fire Safety department was discussing its concerns about the misinterpretation of functional requirement B4, it was also doing work on compartmentation in residential blocks of flats.[490] As it had in relation to the exterior walls of such properties, the department continued to question whether its enforcement powers under the Fire Safety Order extended to the fire-resisting walls between individual flats. That was not a new issue. It had featured in discussions between the LFB and DCLG in 2012, which had culminated in Louise Upton’s advice of 6 February 2013 that the Fire Safety Order did not extend to the external walls of a building.[491] In August 2016, Andrew Jack produced a report entitled Fire Resisting Compartmentation – Flats (the Jack report) that was presented to the Principal Management Board, a departmental management board chaired by AC Daly and attended by the heads of the different teams in Fire Safety.[492] The Jack report described the benefits of taking enforcement action, where necessary, in respect of inadequate compartmentation, even though its power in law to do so was considered to be unclear. It noted that compartmentation between flats was of vital importance to prevent the spread of fire through a building containing multiple dwellings and was essential if an evacuation strategy based on “defend in place” was to be employed.[493] (“Defend in place” is essentially the same as a “stay put” strategy.)
Mr Jack observed that fire risk assessments rarely consider compartmentation in areas of the building away from the means of escape and that there was therefore scant factual basis to justify the use of a “stay put” emergency plan.[494] That reflected the fact that a “stay put” strategy for any building is fundamentally dependent on compartmentation being effective and that, in order to rely on “stay put” as a strategy, the building’s compartmentation must be sound. It also follows that, from an operational perspective, it cannot be assumed that compartmentation will in fact be effective.
The Jack report contained examples of buildings whose compartmentation had been found to be inadequate, including Lakanal House, and noted that more examples were likely to be discovered as a result of fire risk assessments.[495] AC Daly said that a great deal of the LFB’s enforcement work concerned breaches of compartmentation and that his own operational experience had been that it was often possible to find products of combustion where you would not expect them.[496] However, he did not accept that the LFB had reason to think that inadequate compartmentation was a widespread problem.[497] It is also clear that no thought was given by the LFB at that stage to the potential combination of inadequate compartmentation and combustible facade systems, even though the report was being written while Bureau Veritas was carrying out tests on the panels taken from Shepherd’s Court.[498] The Fire Safety department did not take the opportunity to raise its concerns about inadequate compartmentation in the letter it sent to chief executives on 6 April 2017. This might have been due to the fact that compartmentation had been effective at Shepherd’s Court, thereby keeping the single staircase clear of smoke and fire and enabling the partial evacuation of residents.
On 3 April 2017, Commissioner Cotton wrote to the then Gavin Barwell MP, Minister of State for Housing and Planning and Minister for London, requesting a meeting to discuss the LFB’s concern about inadequate compartmentation in residential blocks of flats.[499] In her letter she pointed out that effective compartmentation is essential to the operation of the “stay put” policy that applies to most residential buildings. She expressed concern that since the beginning of 2017 the LFB had identified, on average, at least one residential property (or development) a month in London that had significant defects in compartmentation and that there were many other cases that had not come to the LFB’s attention.
Commissioner Cotton told us that the letter had been drafted by AC Daly and that she had not been aware of the problems to which it referred before he had spoken to her about the draft.[500] She did not take any steps to check what training was being provided to operational personnel about the risks posed by failures of compartmentation or their effect on a building’s “stay put” strategy.[501]
By the end of 2016, the LFB as an organisation was well aware of the dangers posed by some kinds of modern construction materials and techniques and of the particular dangers presented by various kinds of combustible materials, mainly those used for their insulating properties. That included sandwich panels, insulation boards made of organic materials and, most importantly for present purposes, external panels containing organic materials intended to provide rigidity as well as insulation, all of which had the propensity to lead to a loss of compartmentation in a major fire. Regrettably, however, that knowledge was almost entirely confined to the Fire Safety department and was not shared with those who were responsible for operations. As a result, those who were deployed to fight fires were not trained to deal with situations which could become catastrophic both for them and, in the case of residential buildings, their occupants. In particular, incident commanders were not sufficiently aware that a “stay put” strategy may not be reliable in all circumstances and that evacuation may be necessary.
In his Phase 1 report the chairman found that the information available to the first crews mobilised to attend the Grenfell Tower fire was incomplete and in some respects inaccurate.[502] He also found that the LFB had failed properly to train its crews in how to obtain information when visiting premises for that purpose and had a narrow understanding of its obligations under section 7(2)(d) of the Fire and Rescue Services Act 2004 (the 2004 Act).[503] He said that the reason for those failures would be investigated in the next phase of the Inquiry. We have therefore examined the LFB’s approach to operational planning, with particular reference to fighting fires in high-rise residential buildings.
Section 7(2)(d) of the 2004 Act requires fire and rescue authorities to make arrangements for obtaining information needed for the purpose of extinguishing fires and for protecting life and property in the event of fires in their areas. Traditionally, visits by station-based staff to premises in their areas have been regarded as the primary means of discharging that duty and was the method adopted by the LFB.[504]
Information gathered from visits to premises and other sources was entered on the Operational Risk Database (ORD) which was intended to act as the main source of information for incident commanders and other officers responding to an incident. In his Phase 1 report the chairman considered the entries on the ORD for Grenfell Tower, which indicated that the LFB had failed to obtain relevant information from the manager of the building, the TMO, including information relating to the building’s cladding system.[505] Contrary to the plain meaning of the words of Appendix 1 of PN633, it was not the practice for operational personnel responsible for conducting visits to high-rise premises to consider the full list of items set out there.
In Phase 2 of the Inquiry we have considered what information section 7(2)(d) requires fire and rescue services to gather and how the LFB sought to discharge its duty, including the type of information it thought it needed to obtain, particularly about high-rise residential buildings. We have also considered whether the LFB’s policies and practices that were designed to discharge the duty under section 7(2)(d) were appropriate.
The duty to obtain information for the purpose of fighting fires was originally contained in section 1(1)(d) of the Fire Services Act 1947, which was to all intents and purposes the same as section 7(2)(d) of the 2004 Act. Steve McGuirk, the former Chief Executive and County Fire Officer of Greater Manchester Fire and Rescue Service, who was called to give expert evidence on fire-fighting, explained that the duty had originally been interpreted by fire and rescue authorities as requiring the collection of simple information that would be readily and quickly accessible to the first crews attending an incident,[506] and that had remained their approach to discharging the duty under section 7(2)(d) of the 2004 Act.[507]
In April 2012, the government issued guidance to fire and rescue services on the collection and management of operational risk information, that is, the information they are required to collect under section 7(2)(d).[508] It contained a model approach entitled Provision of Operational Risk Information System, or PORIS for short. It was the first substantive national guidance on the management of operational risk information since the 2004 Act had come into force.[509] Mr McGuirk said that PORIS had marked a change in what was expected of fire and rescue authorities because it required a much more sophisticated system for managing information about risks, but he doubted whether it had brought about a widespread change in the way that most fire and rescue authorities went about gathering information. That may have been because the guidance was released with little publicity, but in any event, there has been no monitoring of whether any, and if so, how many, authorities have adopted the model.[510]
The PORIS model involved five steps: (1) review existing information; (2) where necessary, collect additional information by way of a site visit; (3) use that information to assess the risk presented by the particular building or site; (4) determine the appropriate risk management process; (5) provide the relevant information for use by incident commanders in a timely manner. The guidance provided a template “data capture” form, to be used for the collection of information, including information collected during visits to premises.[511] It is notable that the form included a section entitled “cladding and roof” and invited the user to select from a number of different alternatives, including “sandwich panel”, “metal sheet” and “uPVC”.[512]
It is immediately apparent when looking at the data capture form (which is almost 20 pages long, extremely broad in scope and in parts very technical) that the guidance issued in 2012 envisaged a process for the collection and management of operational risk information very different from the simple and practical approach that had previously been adopted by fire and rescue authorities. Mr McGuirk described the guidance as prescribing a much more expansive approach which required a significant amount of additional training.[513] Following the introduction of PORIS, as Mr McGuirk put it, operational firefighters were intended to become “more rounded risk assessors, capable of assembling and evaluating a much greater range of information.”[514]
The LFB policies for the management of operational risk information were PN800, which applied to all properties, and PN633, which related specifically to high-rise buildings. Appendix 1 of PN633 contained a list of 22 items to be considered by crews during section 7(2)(d) visits.[515] In addition, PN784 governed the sharing of information relevant to operational planning between the LFB’s Fire Safety department and fire stations.
In broad terms, the version of PN800 in force in June 2017 mirrored the five stages of the PORIS model. In particular, it required crews to carry out a premises risk assessment based on the risks identified during section 7(2)(d) visits using the form in Appendix 1 of the policy. That resulted in the premises achieving a certain risk score, which determined the frequency of further visits, the need for exercises on the premises and whether a tactical plan was required. Grenfell Tower had been placed in the medium- to low-risk category by the risk assessment carried out at the last visit before 14 June 2017. As a result, it qualified for at least one visit by a local crew every three years and a tactical plan. An exercise on the premises was not required unless the local station manager thought it necessary.[516] No tactical plan was ever put in place for Grenfell Tower.[517]
PN800 recognised the role of the LFB’s Fire Safety department in the collection, management and analysis of operational risk information. In particular, the policy noted that one of the ways in which premises giving rise to certain hazards or risks were identified was by notification from the Fire Safety department. PN800 also directed crews to consider whether the risk assessment process required specialist knowledge, including knowledge available from the Fire Safety Regulation department.[518]
PN784 governed the way in which information was to be shared between the Fire Safety team and operational crews.[519] In short, PN784 set out a procedure under which officers in the Fire Safety department were to communicate to station-based personnel information likely to be relevant when planning for operational incidents, and vice versa. Such information was to be communicated in a prescribed form and, on receipt, the station manager or Fire Safety team leader was to decide what action was appropriate, which might include a joint visit.
In practice, the procedure for sharing information between the Fire Safety department and fire stations was not consistently followed. Reports were compiled by the Director of Operations on a quarterly basis showing the number of “risk notifications” made by the Fire Safety department to stations during that period and the action taken by the relevant stations in response. We have been provided with a copy of one of those reports, dated 12 May 2015.[520] It records that in Kensington and Chelsea, where Grenfell Tower was situated and which contained three fire stations,[521] the Fire Safety department had made a total of six notifications to fire stations in the previous year and just two notifications had been made by fire stations to the Fire Safety department. More generally, the proportion of notifications in respect of which follow-up action was recorded varied from station to station, with some recording 100% and others as low as 40%. The report noted that the Fire Safety department sent more notifications to the stations than the stations sent to the department, which could have been the result of the stations not being fully aware of the administrative recording process, alternative channels of communication for recent team management changes or differences of opinion about the level of information that should be referred. The Fire Safety department made similar observations.[522]
The picture recorded in the report of 12 May 2015 was consistent with the evidence of AC Daly. He said that on the whole, the flow of information between the Fire Safety department and the fire stations did not work well and was patchy, in the sense that it worked better in some areas than others.[523] Both Commissioner Dobson and Commissioner Roe agreed with that assessment.[524] The LFB’s Director of Operations, Dave Brown, said that the LFB had put measures in place to address the shortcomings in the system which had led to improvements.[525] Whatever measures had been implemented, they were ineffective, because the sharing of information between the Fire Safety department and fire stations remained unsatisfactory at the time of the Grenfell Tower fire. AC Daly was a frank and reliable witness, who had much closer contact with the day-to-day management of the Fire Safety department than Director Brown. On this point, we prefer AC Daly’s evidence. Indeed, Grenfell Tower was a tragic illustration of the failings in the LFB’s arrangements for sharing information. The North Kensington crews who carried out section 7(2)(d) visits to the tower did not obtain from the TMO information relating to the building’s cladding system or even basic floor plans showing the layout and numbers of individual flats. Under the LFB’s own policies and procedures that information should have been obtained by the local crews.
Neither PN800 nor PN784 provided any direction or guidance on the management of operational risk information relating specifically to high-rise buildings, which at the time of the Grenfell Tower fire was contained in PN633, the LFB’s policy on firefighting in high-rise buildings. PN633 was considered in some detail in Phase 1 of the Inquiry. Appendix 1 of PN633 transposed national guidance on firefighting in high-rise buildings, contained in GRA 3.2, into the LFB’s local policy, insofar as the collection of operational risk information was concerned. Specifically, the LFB’s list of items to be considered during visits to high-rise buildings broadly corresponded to that prescribed by GRA 3.2, apart from the omission from Appendix 1 of any reference to cladding.[526]
Mr McGuirk thought that it would take an operational crew at least two hours properly to consider all 22 items listed in Appendix 1 of PN633.[527] He disagreed with Commissioner Cotton’s characterisation of the list as being, in parts at least, unrealistic or incorrect. In his view, it was necessary and appropriate for crews in London to be directed to consider all 22 items as well as the information required by the PORIS model. He did not think it was beyond the capacity of station-based operational crews to undertake risk assessments of that scope and level of detail, provided they were given appropriate training. In his opinion, the practical simplicity of the former approach to management of operational risk information can still be maintained, thereby preserving the need for essential information to be readily available to the first responding crews, if measures are taken to filter the information properly as it is provided to those on the incident ground.[528]
The LFB’s policy documents did not make it clear whether all high-rise buildings should be the subject of section 7(2)(d) visits and have an entry on the operational risk database or only some. AC Brown said that ideally every high-rise building in London would be visited and subject to a risk assessment, a view with which Commissioner Dobson agreed.[529] However, that might or might not have led to their being recorded on the ORD, since PN800 prescribed a minimum threshold risk score for that purpose.[530] AC Brown accepted that he had faced considerable difficulties in achieving that ideal during his time in the brigade, not least because the LFB did not know, and had no obvious means of finding out, how many high-rise buildings there were in London and where they were situated.[531]
The figures that have been provided to us indicate that the LFB was a long way from achieving AC Brown’s ideal. The Lakanal Assurance Report, a review carried out by the LFB in August 2018 of the action taken in response to the Lakanal House fire, recorded that in October 2017 approximately 1,700 high-rise buildings had been subject to a risk assessment out of a total of about 6,900 such buildings in London.[532] The LFB has since confirmed that the total number is in fact about 8,500.[533]
The reason why such a low number of high-rise buildings appeared on the ORD might have been the apparent confusion within the LFB over whether crews were expected to visit all high-rise buildings on their ground and, if not, which ones they were expected to visit. AC Brown sent an email to station managers in April 2009 directing them to ensure that crews visited all the high-rise buildings on their ground every year.[534] His recollection was that, at that time, he had felt that that was not an unreasonable expectation, because he had not been quite sure how many there were. At a later stage, however, when the magnitude of the task became more apparent, a more risk-based approach was adopted.[535]
It appears that AC Brown’s instructions still stood in 2010, when PN633 underwent one of the several reviews that were carried out following the Lakanal House fire. Peter Cowup, who was then a DAC in the LFB’s Operational Policy department and was leading the review of PN633, sent an email on 1 August 2010 to various senior officers within the LFB noting that the feasibility of crews visiting all high-rise buildings on their station’s ground required further consideration, because of the size of the task, especially for stations in central London.[536]
In November 2011, the LFB published Operational News 20, which contained an article on high-rise firefighting. In that article personnel were told that any high-rise buildings which posed a particular risk should be the subject of section 7(2)(d) visits.[537] AC Brown denied that the article reflected a departure from his earlier direction that all high-rise buildings should be visited. He said that the article had been intended to refer to the fact that high-rise buildings would be subject to regular section 7(2)(d) visits in future only if they were considered to pose a particular risk after they had been subject to an initial risk assessment.[538] We do not accept that. The text of the article in Operational News is clear and is not qualified in the way he suggested. The article is a straightforward guide for station-based crews on the LFB’s statutory obligations in relation to high-rise buildings. We think that it illustrates the lack of a consistent approach to whether section 7(2)(d) of the 2004 Act required the LFB to visit all high-rise buildings or only those deemed on some undefined basis to present a high risk.
As has been noted, Appendix 1 of PN633 listed 22 items which crews were required to consider during section 7(2)(d) visits to high-rise buildings. Mr McGuirk and Commissioner Cotton expressed different views about the practicability of complying with Appendix 1 to the letter. From around 2012 until his retirement in March 2017, Director Brown had ultimate oversight of the LFB’s fire stations and responsibility for discharging its obligations under section 7(2)(d).[539] His evidence was therefore of particular help in understanding the nature of the information the LFB expected its operational crews to gather.
AC Brown expected crews to use the list in Appendix 1 to PN633 as an aide memoire and to consider the items where practicable. He accepted that that was not reflected in its language, which required crews to ensure that they were familiar with the various items contained in the list.[540] However, he did not think that station-based crews had the technical knowledge to look in depth at factors that might give rise to breaches of compartmentation, despite that being one of the items mentioned in the list. He said that, leaving aside obvious problems, such as an open vent in a communal stairwell, it was beyond the skill and knowledge of operational crews to identify defects likely to have that effect.[541] Similarly, when asked whether he would expect crews to identify features of a building that might promote the rapid or abnormal spread of fire (another item in the list) AC Brown said that that was at the extreme of the knowledge to be expected of a firefighter and that the LFB would rely on a member of the Fire Safety department to identify features of that kind.[542] Commissioner Dobson was similarly sceptical. He said that some of the items in the list would have required very specialist training to enable crews to carry them out properly. He doubted the likely benefit of such training in any event.[543]
AC Brown did not expect crews to look at a building’s cladding system during a section 7(2)(d) visit or to decide whether it should be taken into account in the risk assessment.[544] Again, he thought that was beyond the ability and training of operational personnel.[545] There was no discussion internally following the Lakanal House fire about whether to direct crews to consider cladding systems,[546] despite the fact that Commissioner Dobson had been sufficiently concerned about unsuitable panels to write to Sir Ken Knight on the subject in December 2009.[547] AC Brown told us that other steps had been taken to deal with that, which did not involve operational firefighters in that level of detail.[548] Nor was any consideration given to requiring crews to collect information about cladding systems of high-rise buildings following the fire at Shepherd’s Court in August 2016.[549]
The lack of any advice or direction to crews about how to carry out visits to high-rise premises for the purposes of section 7(2)(d) is clear from the operational risk information training materials that were provided to the Inquiry, which were limited to a single, interactive computer-based training programme produced by Babcock in around May 2013.[550] AC Brown confirmed that that was the first time crews had received formal training on how to conduct such visits,[551] and we are satisfied that it was the only time. The package was not directed specifically to high-rise buildings and did not contain any reference to PN633. Although it did provide some commentary on what to look for on such a visit, that commentary did not address the risk of fire spreading beyond the compartment of origin or the existence of features of construction that might promote the rapid or abnormal spread of fire, both of which are included in the list contained in Appendix 1. Perhaps unsurprisingly, the training did not ensure that crews understood the purpose of their visits, nor what information they were expected to obtain and record. That is apparent from the deficiencies in the ORD entry for Grenfell Tower, considered in detail in the Phase 1 report.[552] Although AC Brown and DAC George sought to suggest otherwise,[553] Commissioner Roe confirmed that such deficiencies were not confined to Grenfell Tower, as might be expected.[554] He told us that a review of the entries on the ORD carried out after the Grenfell Tower fire had revealed a range of inconsistencies, poor information and a misunderstanding of risk.[555]
The LFB’s failure, following the Lakanal House fire, to instruct operational crews visiting premises pursuant to section 7(2)(d) to consider the potential for widespread compartmentation failure and the rapid or abnormal spread of fire was significant. It is not sufficient for it to point to measures that might have been taken by the Fire Safety department if the concerns of senior officers had been brought to its attention. Operational crews were not provided with the direction or training to enable them to identify the matters that should have been reported and largely disregarded the system for sharing such information.
The publication of PORIS in April 2012 provided another opportunity for the LFB to review and consider the effectiveness of its processes for the management of operational risk information. On 27 February 2013, a report by Susan Ellison-Bunce, Head of Strategy and Performance, was submitted to the Corporate Management Board, which considered the new guidance and the extent to which the LFB complied with it.[556] She concluded that the existing processes were robust and largely complied with national guidance and that it was not necessary or practicable to make significant adjustments to the current arrangements.[557]
Ms Ellison-Bunce also noted that the national guidance referred to the importance of periodic audits as a means of monitoring whether operational risk management systems had been properly implemented and maintained and were effective in meeting their objectives. She found that there were inconsistencies in the approaches taken by stations to what was included on the ORD and that the quality of the work done in obtaining and using information varied. Ms Ellison-Bunce therefore recommended that the Head of Operational Assurance (then AC Cotton) review how stations identified sites and buildings that might present a risk and whether they adopted an approach consistent with PN800.[558] AC Brown told us that that review had not been carried out.[559]
In her Rule 43 letter to the LFB the coroner recommended that it review its procedures for sharing information obtained pursuant to section 7(2)(d) with crews both within the station in question and at other local stations.[560] In response the LFB created a regime for inspecting what Commissioner Dobson had referred to in his letter to the coroner of 23 May 2013 as “high priority” buildings, with a view to increasing the number of premises in respect of which information was available on the ORD.[561] The term “high priority” did not appear in either PN800 or PN633. AC Brown told us that he did not know where it had come from and thought it had caused some unnecessary confusion.[562] The purpose of the new regime was to identify buildings that had not been the subject of a risk assessment but should have been.[563] It was not specifically aimed at high-rise buildings, but they were regarded as a priority.[564] AC Brown wanted to create an inspection regime that resulted in more entries on the ORD and was concentrated on those that presented higher risks.[565]
In November 2013 AC Brown asked DAC Tom George to set up the new regime, but he immediately delegated the task to GM John Elwell.[566] DAC George provided GM Elwell with little guidance on what was required, apart from telling him that he needed to strengthen the inspection programme and increase the number of entries on the ORD.[567]
On 11 December 2013, GM Elwell produced a careful and considered report for DAC George and AC Brown,[568] in which he identified the following questions that he thought were raised by the concern that there were too few entries on the ORD:
The questions identified by GM Elwell demonstrated a perceptive understanding of the difficulties that beset the LFB’s systems for the collection and management of operational risk information. Indeed, they foreshadowed many of the concerns that have been raised during this Inquiry, in particular, about the capacity of individual stations to manage the number of premises on their grounds effectively, the quality of the existing entries on the ORD and the competence of operational staff to carry out visits and record relevant information.
When he came to deliver his report[569] and recommendations GM Elwell concentrated on the following:
AC Brown’s response to the report was that, although it was interesting and helpful, it did not amount to the creation of a high priority inspection regime.[571] He accepted that the report had raised some significant broader concerns about the adequacy of the LFB’s existing arrangements, but he told us that some of the recommendations had either been implemented already, were in the course of being implemented, or were within GM Elwell’s power to implement. He thought that one or two were very aspirational and, although desirable in principle, would not work in practice.[572]
AC Brown thought that discussions between managers about section 7(2)(d) visits were an established part of normal business and that nothing further needed to be done in that respect.[573] He said that work had already been done by the LFB’s Information Management department to link information obtained from previous section 7(2)(d) visits with data available from other internal sources, including the Fire Safety department. He did not think that there could be a review of the varying levels of risk across different stations because the LFB did not have the necessary information. It could therefore not determine an optimal number of entries on the ORD for any individual station; all it could do was to direct crews that in due course all premises should be inspected to determine their suitability for inclusion on the database. He was satisfied that training on section 7(2)(d) visits had recently been given to crews (meaning, the training package distributed in May 2013)[574] and considered that the LFB needed first to assess the results of that training in order to determine whether more was required. When asked about the need to monitor the quality as well as the quantity of the entries on the ORD, he said that it was incredibly difficult to measure quality in any meaningful way.[575]
We are unable to accept that AC Brown carefully considered each of GM Elwell’s recommendations when the report was presented to him in late 2013. The weight of the evidence shows that he was concentrating on the introduction of an inspection regime aimed at “high priority” buildings, however defined. We think that he rejected the recommendations because they were not directly related to the creation of such a regime. In so doing, he did not properly reflect on the very real concerns that had been raised by GM Elwell.
We gained the strong impression that AC Brown did not wish to become involved in considering the complexities of an inspection regime, a problem which deserved more careful consideration than he was willing or able to give it. If the letter and spirit of the coroner’s recommendation were to be satisfied and more effective inspection arrangements introduced, the matters raised by GM Elwell required proper consideration. AC Brown failed to give them that consideration and, as far as we can see, there was no good reason for that. If GM Elwell’s recommendations had been implemented, they could have gone some way towards remedying the deficiencies in the LFB’s arrangements for gathering and managing operational risk information.
On 22 January 2014, following AC Brown’s effective rejection of GM Elwell’s report, DAC George compiled a list of different types of property for inspection in order of priority that he proposed should be given to station managers and borough commanders.[576] High-rise residential buildings of six floors and above appeared on the list second only to sites such as industrial plants of a kind which present major accident hazards. A list of that kind was exactly what AC Brown wanted.[577] DAC George said, however, that in his view and that of his colleagues, a satisfactory banding system was not entirely achievable and that he had reservations about such a simplistic approach.[578] In particular, he was concerned that the system was more concerned with numbers than quality and that it would be virtually impossible for crews to carry out meaningful inspections of such a large number of premises.[579] AC Brown did not agree with DAC George’s reservations[580] and on 24 May 2014 he sent an email to all operational crews directing them to have regard to the priority banding system when conducting section 7(2)(d) visits.[581]
The priority banding system was never formally incorporated into any policy,[582] but DAC George told us that he had monitored its implementation by watch managers through regular meetings with the borough commanders beneath him in the LFB’s organisational structure. AC Brown had no further involvement in the inspection regime and did not ask to be provided with any further information about its success in increasing the number of entries on the ORD or its progress generally.[583]
The references in PN800 to factors liable to affect communications were confined to circumstances likely to be encountered underground or in other places which may have alternative communications infrastructure, including fixed radio repeaters. However, the list of matters in Appendix 1 to PN633 on high-rise firefighting that were to be considered on visits to high-rise buildings did include potential problems with communications.[584]
The evidence given in Phase 2 about the practical application of those policies was inconsistent and uncertain. In particular, senior officers did not clearly understand whether there was a need to test the performance of radios when visiting a high-rise building.[585] PN633 contained no guidance for crews on how to identify potential difficulties with communications or how to test radio reception reliably.[586] Although WM Ricketts from North Kensington fire station tested the transmission of radio signals between the basement and the ground floor using his handheld UHF radio during a visit to Grenfell Tower immediately before the fire, that could have given only a limited indication of the performance of radios in the tower under operational conditions.[587] Professor Johnson suggested that a more detailed test, using validated procedures, may be needed in structures known to pose a particular risk of deteriorating communications.[588]
The Generic Risk Assessments were published by the Chief Fire and Rescue Adviser in conjunction with DCLG to provide operational guidance to fire and rescue authorities. In his Phase 1 report the chairman described the purpose of Generic Risk Assessment (GRA) 3.2, which contained the national guidance on firefighting in high-rise buildings, as being to assist fire and rescue services in drawing up their own assessments of risk to meet their statutory obligations under the relevant Health and Safety at Work legislation.[589] The provisions of GRA 3.2 that are most relevant to the hazards encountered at Grenfell Tower were identified in the Phase 1 report.[590] In summary, they relate to planning, training and competence, and the provision of fire survival guidance.
Individual fire and rescue services are obliged to have regard to national guidance when carrying out the risk assessments which underpin their operational policies.[591] The LFB’s policy on high-rise firefighting was PN633; the version published in June 2015 was in force at the time of the Grenfell Tower fire.[592]
The second version of GRA 3.2 had been published in 2008, and in 2010 a review of the full GRA series was commissioned by DCLG and the Chief Fire and Rescue Adviser.[593] Although DCLG in conjunction with the Chief Fire and Rescue Adviser had final editorial control of the series as a whole, DCLG retained particular responsibility for the contents of GRA 3.2.[594] The review process began in 2010 and culminated in a revised version published in 2014.[595] DCLG delegated the management of the review to Surrey Fire and Rescue Service under the terms of a memorandum of understanding,[596] but oversaw the process through a strategic management board established for the purpose.
The review of GRA 3.2 was given priority over the work on other Generic Risk Assessments because it was thought that important insights had been gained into fighting fires in high-rise buildings as a result of the experience at Lakanal House.[597] In March 2011 the LFB was appointed to lead the work on GRA 3.2; no other fire and rescue service was involved in the drafting.[598] The LFB was seen as the appropriate organisation to take on that role because much of the learning that needed to be incorporated into the guidance had been derived from the Lakanal House fire.[599] The close involvement of the LFB in the revision of GRA 3.2 gave it a unique opportunity to gain a deep understanding of the risks to which firefighters and members of the public may be exposed in such situations, particularly in buildings that have been constructed using novel products and modern materials and methods of construction. It is therefore worth considering in a little detail the way in which the revision of GRA 3.2 proceeded and the extent to which the guidance it contained was reflected in the revision of the LFB’s own policy on fighting fires in high-rise buildings.
Within the LFB, DAC Cowup was given primary responsibility for producing the revised version of GRA 3.2 with support from members of the Operational Policy department.[600] In December 2011, he and his team produced a draft revised version of GRA 3.2,[601] which was then the subject of a regional and national consultation until September 2012.[602] The draft was revised during the course of that process to reflect some of the responses that had already been received. At that stage, DAC Cowup was confident that it fully reflected the lessons to be learnt from the Lakanal House fire, subject to the findings of the inquests which were due to start in January 2013.[603]
The draft produced during the consultation period contained new sections on evacuation and handling fire survival guidance calls. It contained the same direction to the incident commander to follow any evacuation plan devised as part of the occupier’s fire risk assessment,[604] but there was no express reference to the potential need to carry out an evacuation of a residential building with a “stay put” strategy. In particular, the oblique reference to the “stay put” principle did not accurately reflect the national guidance that residents are usually safest remaining in their property unless affected by fire, heat or smoke (whatever the source).[605] There was also no reference to the need to re-evaluate the advice being given to callers during the course of an incident or to the possibility that “stay put” advice might have to be reversed.
DAC Cowup did not accept that he and his team had failed to consider the potential need to revoke “stay put” advice during the course of an incident at a residential high-rise building. On the contrary, he said that they had recognised that it was one of the lessons of the Lakanal House fire. Although he accepted that the draft was not as explicit as it might have been, he thought that people would have understood that to be necessary, having seen the reference to the need to change the evacuation strategy if and when the situation made it appropriate.[606]
Following the Lakanal House inquests, DAC Cowup was provided with copies of the coroner’s rule 43 letters to the LFB and DCLG, which contained recommendations relating to section 7(2)(d) visits and incident command training. He examined them to ensure that all the points raised in the letters had been covered in the draft revision of GRA 3.2.[607] That exercise resulted in further changes to the text, but he did not think that any substantial amendments were required.[608]
The section relating to handling fire survival guidance calls was changed, however, by the addition of a direction to re-evaluate the caller’s situation from time to time to ensure that the balance of risk between leaving the building and remaining in place was reconsidered as circumstances changed.[609] An amendment to that effect was ultimately included in the published version of GRA 3.2 and was also incorporated into the edition of PN633 published in 2015.[610] The oblique reference to the “stay put” principle was also changed so that it was consistent with the advice contained in national guidance and PN790,[611] but no reference was made to the potential need to carry out an evacuation of a high-rise residential building with a “stay put” strategy.
In his response to the coroner’s rule 43 letter to his department, the Secretary of State for Communities and Local Government had given a clear undertaking that the revised version of GRA 3.2 would include advice to incident commanders to help them make decisions on evacuation if it became clear during an incident that a “stay put” strategy was no longer tenable.[612] DAC Cowup could not recall having seen the Secretary of State’s letter.[613] None of the witnesses who gave evidence to the Inquiry, including those who had worked for DCLG at the time, was able to explain why that was so, despite the letter’s obvious relevance to the work on GRA 3.2.
After the Lakanal House inquests ended in March 2013, DCLG officials became involved in the review of GRA 3.2 at what was intended to be the final stage of the preparation of the revised version for publication. Their involvement led to the incorporation of much of the significant new content, including provisions on the need for an evacuation plan and for incident commanders to be able to evacuate buildings with “stay put” strategies.
On 19 June 2013, representatives of the LFB and DCLG met to put the finishing touches to the draft. No one raised any concerns about the text.[614] Following that meeting, however, the draft was reviewed by other officials within DCLG and significant comments were made by Louise Upton, the Head of Fire Safety Policy. In her evidence, Ms Upton said that she had previously known nothing about the review of GRA 3.2, apart from the commitment made in the Secretary of State’s letter and having occasionally received various versions of the draft.[615] Possibly as a result of her distance from the subject matter, Ms Upton drew attention to significant defects in the treatment of the “stay put” principle and other important aspects of firefighting in high-rise buildings. In an internal email sent to a number of her colleagues on 1 July 2013 she concentrated on the extent to which the document satisfied the Secretary of State’s undertaking that the revised version of GRA 3.2 would include advice to incident commanders to help them make decisions about evacuation.[616] In a later internal email sent on 29 July 2013 she expressed the view that a more fundamental review of the document was required. She referred to the work done by the LFB since the Lakanal House fire to revise its own operational guidance and considered it odd that the revised draft GRA 3.2 did not appear to reflect the lessons learnt by the LFB as a result of that fire.[617] In saying that, she clearly thought that the LFB had given consideration to the potential need to evacuate a high-rise residential building.[618]
Another meeting took place on 30 July 2013 to discuss Louise Upton’s concerns. It was attended by DAC Cowup and Philip Morton from the LFB, Les Britzman (a member of the Chief Fire and Rescue Adviser’s team) and Anthony Maude of DCLG and Leigh Brinton, an employee of Surrey Fire and Rescue Service, who was also involved in the review of GRA 3.2.[619] Louise Upton did not attend the meeting because she did not consider that she could contribute on matters relating to operational firefighting. She believed that her concerns would be voiced by Les Britzman.[620]
At the meeting Mr Britzman led the discussion, which concentrated on the treatment of the “stay put” principle.[621] According to DAC Cowup, that was the first time that questions of that kind had been raised by DCLG and he had been deeply frustrated by the fact that substantive changes were being proposed at such a late stage.[622] Nonetheless, his understanding was that the changes were minor rather than fundamental; DCLG did not tell him that he needed to start again.[623] He said that he had not become aware of DCLG’s concern that the draft did not meet the Secretary of State’s commitment to the coroner until he was preparing to give evidence.[624] Although the point may not have been made to DAC Cowup with the same clarity as it had been made in Ms Upton’s emails, the correspondence following the meeting on 30 July 2013 made clear the department’s desire for greater clarity about, and greater emphasis on, the advice to incident commanders about evacuation in order to fulfil the commitment given by the Secretary of State to the coroner.[625]
Following the meeting on 30 July 2013, DAC Cowup and his team made further changes to the draft[626] by adding passages on the need to re-evaluate “stay put” advice during the course of an incident and to change it if circumstances made that necessary (both points that had been identified by DAC Cowup in his response to the coroner’s rule 43 letters).[627] However, the draft still did not mention the need for incident commanders to understand when to carry out an evacuation of a building with a “stay put” strategy or to the need for there to be an evacuation plan if a “stay put” strategy became untenable.
Notwithstanding those revisions, DCLG continued to have misgivings about the draft. On 15 October 2013, Louise Upton said in an email to Les Britzman and others at DCLG that her earlier concerns appeared not to have been particularly well addressed in the revised version.[628] She sent a large number of comments on the draft document to Mr Britzman, including a reference to the need for contingency plans to provide for evacuation,[629] but they were not sent on to DAC Cowup.[630] The substance of Ms Upton’s comment on the need for an evacuation strategy was ultimately retained in the published version of GRA 3.2.
Ms Upton’s comments also included a reference to the need for training to give incident commanders an understanding of when a full or partial evacuation of a residential building subject to a “stay put” strategy might be necessary.[631] Again, her comment ultimately appeared in the published version of GRA 3.2 in substantially the same terms.
Following various discussions, and notwithstanding DCLG’s reservations, the decision was taken to publish the revised GRA 3.2 without any further substantive amendments. The decision followed a conversation between Commissioner Dobson and Peter Holland,[632] Chief Fire and Rescue Adviser, who, DAC Cowup recalled, had also been of the view that they should move towards publication.[633] Within DCLG, however, the document was described by some as a wasted opportunity and “not fit for purpose”.[634]
Be that as it may, GRA 3.2 in its final form clearly contemplated that the total evacuation of a high-rise building should be an important part of any fire and rescue service’s contingency plan for a building and that incident commanders should not assume that compartmentation would invariably be maintained.[635]
In November 2011, the LFB published a revised version of PN633 which reflected changes to the policy considered necessary in the light of the Lakanal House and the Shirley Towers fires.[636] DAC Cowup described it as a comprehensive revision.[637] However, the revised policy contained no reference to the need to make contingency plans for evacuating the whole building, although crews visiting buildings pursuant to section 7(2)(d) of the 2004 Act were directed to have regard to the risk of fire spreading beyond the compartment of origin and the possible need for multiple rescues.[638] There were references to evacuation throughout the policy, including a direction that the incident commander should follow the evacuation plan devised as part of the occupier’s fire risk assessment unless the situation dictated otherwise,[639] but there was no reference to the possibility that a building with a “stay put” strategy might need to be evacuated or indeed any explicit reference to the “stay put” principle at all.
The LFB’s review of PN633 to bring it in line with the revised GRA 3.2 began in early 2013. DAC Cowup asked GM James A’Court, then part of the Operational Policy department, to co-ordinate it.[640] GM A’Court asked SM Patrick Utting, then part of the Incident Management team, to take the lead on drafting the revised policy.[641] DAC Cowup expected GM A’Court and SM Utting to keep him informed about any revisions to the draft GRA 3.2 as work went on and take them into account. He also expected them to have regard to any lessons arising out of the Lakanal House inquests, which had recently begun.[642]
DAC Cowup told SM Utting that transposing the relevant elements of GRA 3.2 into LFB policy was likely to be a relatively straightforward task.[643] He did not recall specifically asking SM Utting to consider the coroner’s rule 43 letters and SM Utting confirmed that he had not been asked to consider them as part of his work.[644] SM Utting was similarly unaware of the contents of the Secretary of State’s response to the coroner or of his commitment to including in the revised GRA 3.2 advice to incident commanders to inform decisions on evacuation.[645]
The version of PN633 produced in 2015 was neither as clear nor as comprehensive as GRA 3.2. In particular, both the risk assessment and the gap analysis that SM Utting had produced for the purpose of his review of PN633 were based on an earlier draft of GRA 3.2 that pre-dated Ms Upton’s comments in relation to “stay put” and evacuation.[646] Further, neither of them contained any reference to cladding as a feature that crews should consider when gathering information, despite its being referred to in both the 2008 and the 2014 editions of GRA 3.2. There was no satisfactory explanation why the revised PN633 did not fully or accurately reflect the 2014 edition of GRA 3.2 on these important points.
In the section dealing with competence and training GRA 3.2 advised that incident commanders should understand when an evacuation strategy might become necessary in a residential building where a “stay put” strategy is normally in place. That was transposed into paragraph 7.46 of PN633 and to that extent, therefore, the policy did reflect a recognition that compartmentation may fail and that the incident commander may need to carry out a partial or total evacuation of a building subject to a “stay put” strategy.[647] However, no guidance was provided about when or how a decision of that kind should be made. SM Utting doubted whether it was feasible to include in a policy advice that would apply in all situations.[648] That may be so, but it does not explain why no attempt was made to identify factors that might indicate to an incident commander that “stay put” advice should be withdrawn and an evacuation of some nature carried out. In those circumstances, it is not surprising that PN633 did not refer to the need to train incident commanders to recognise the need to withdraw “stay put” advice and carry out an evacuation.[649] but no request for training was initiated in conjunction with the revision of PN633.[650] As Commissioner Roe accepted, at the time of the Grenfell Tower fire the LFB did not provide any guidance or direction in either its training or its policies about when and how a “stay put” strategy should be reversed.[651]
The guidance in GRA 3.2, to the effect that contingency plans for individual premises should cover the spread of fire beyond the compartment of origin and the possible need for multiple rescues, found its way into paragraph 4.8 of PN633, but without any specific reference to the need for a contingency plan. There was no reference to the need for an operational evacuation plan that could be implemented if a “stay put” policy became untenable.[652] SM Utting was unable to explain why that particular aspect of GRA 3.2 had not been incorporated into PN633.[653] DAC Cowup told us that he had understood the phrase “contingency plans” in GRA 3.2 to relate only to high-risk premises, such as national heritage sites or landmark high-rise buildings, and that it would not be practicable to have individual contingency plans for every high-rise building in London.[654] SM Utting expressed a similar view.[655] However, that is not the natural meaning of the expression as it appears in GRA 3.2, where it appears to refer to all high-rise buildings. Although it might not have been practicable to require crews to draw up individual contingency plans for all high-rise buildings, GRA 3.2 required fire and rescue services to consider generally whether and how contingency plans could assist crews and incident commanders. The stark conclusion is that PN633 did not properly reflect the requirements of GRA 3.2 in that respect.
The history of the revision of GRA 3.2 and the review of PN633 is of interest primarily for the light it sheds on the attitude of the LFB to the need to prepare for the evacuation of high-rise residential buildings subject to a “stay put” policy. The need to prepare contingency plans for an evacuation was included in GRA 3.2 as a result of the insistence of officials at DCLG rather than at the instigation of the LFB. The review of PN633 failed fully to reflect the current version of GRA 3.2, possibly because those at the LFB responsible for it did not think that the LFB needed such detailed advice and guidance or possibly because they did not attach sufficient importance to it. Whatever the reason, the close involvement of the LFB in the revision of GRA 3.2, coupled with the critical intervention of officials at DCLG, should have made it clear that producing contingency plans for a full evacuation was an essential part of fighting fires in high-rise buildings. Regrettably, however, that message was not properly absorbed by senior managers, and as a result operational firefighters were not properly prepared to deal with another major failure of compartmentation when it eventually occurred at Grenfell Tower.
The Grenfell Tower fire presented the control room and all those who worked there with a challenge of unprecedented proportions. All those present on that night did what they could to deal with the huge volume of emergency calls and to pass vital information to the incident ground. However, mistakes were made, as described in the Phase 1 report, mainly as a result of inadequate training. It was therefore important for us to examine the way in which the control room had been run and its staff trained in the years immediately preceding the fire, to ensure, as far as possible, that a similar situation does not arise in the future.
The control room lies at the heart of the LFB’s response to fires and other unexpected events as a result of which people’s lives are at risk. It takes emergency calls from the public, despatches fire appliances to incidents and maintains communications with the incident ground. A description of its organisation and method of operation at the time of the Grenfell Tower fire is contained in chapter 7 of the Phase 1 report.
It is important to note at the outset that control room officers (CROs) are not merely call-handlers. As part of responding to emergency calls, they provide fire survival guidance when circumstances require. When providing fire survival guidance, a CRO becomes a first responder, giving critical advice to someone facing a life-threatening situation. Their role is, therefore, complex and proper performance of their functions is critical to the effective operation of the LFB. It depends on effective management of the organisation and the maintenance of critical skills through regular training.
Before 2015, responsibility for the operation of the control room lay with the Operational Prevention and Response department, itself part of the Deputy Commissioner’s directorate.[656] When in 2015 the Deputy Commissioner’s directorate was abolished, that responsibility was transferred to the newly formed Directorate of Operations.[657] From 2015 until 2017, the Director of Operations was AC Brown. From March 2017, AC George took over as Director of Operations.
Until 2011, CROs were divided into four watches covering two shifts within a 24-hour period.[658] Each watch comprised 16 CROs and seven senior control officers under the command of a control commander.[659] Two senior operations managers (SOMs) managed two watches each and held certain other responsibilities which are discussed below. From 2010, the two SOMs were SOM Joanne Smith and SOM Lindsay Turner.[660] They were supported by assistant operations managers (AOMs). In overall command of the control room was the principal operations manager (POM), Scott Hayward.
In addition to the watches staffing the control room, there were two support teams, each led by one of the SOMs. SOM Smith led the Technical Support Group, made up of one OM and two AOMs. SOM Turner led the Training team, made up of one OM and three AOMs. The Technical Support Group was responsible for ensuring that the systems used by the control room, including the mobilising system, were suitable for their purpose and capable of carrying out the functions required to enable CROs to do their work.[661] The Training team was responsible for developing core training and delivering it to CROs.[662] Its members were full-time trainers, although they were not trained as such. All of them were experienced CROs.[663]
In April 2011, the shift pattern was changed. Instead of operating two shifts over 24 hours, CROs worked one of four shifts: a 12-hour day or night shift, or one of two overlapping ‘short’ shifts of eight hours.[664]
At about the time that the shift pattern was changed, the Technical Support Group and the Training team were merged to form a single team known as the Operational Support Team.[665] Although the rest of the control room operated a shift system, the Operational Support Team, as a support body, operated only during the day shift.[666] The Operational Support Team trained CROs while the latter were ‘on watch’, i.e. when their watch was on duty, but during periods when they were not required to undertake control room duties.[667] Training was occasionally provided to CROs outside normal working hours.
The newly formed Operational Support Team contained five AOMs, later reduced to four.[668] Within the Operational Support Team, the members of the former Technical Support Group retained their previous responsibilities and continued to report to SOM Smith.[669] Those officers responsible for training reported to SOM Turner.[670] SOM Smith said that following the merger no one person had been formally placed in charge of the Operational Support Team and that she and Lindsay Turner had shared that responsibility.[671]
In September 2012, SOM Smith was seconded to the Chief Fire Officers Association.[672] At around the same time, SOM Turner left the control room for medical reasons.[673] As a result, Victor Bagnelle and Keith Diamond were temporarily promoted to SOMs, replacing SOM Smith and SOM Turner respectively.[674]
In 2015, the LFB changed its mobilising system from one known as ‘ProCAD’ to a system known as ‘Vision 4DS’. The introduction of a new mobilising system meant that between 2013 and 2015 the Operational Support Team had to design, prepare and deliver intensive training to enable the CROs to use it.[675]
In January 2015, SOM Smith returned from her secondment and assumed overall responsibility for the Operational Support Team.[676] She continued to hold that responsibility until January 2020.[677]
POM Hayward was in day-to-day command of the control room and reported directly to an Assistant Commissioner. Inevitably, the position held by that Assistant Commissioner within the LFB structure varied over time.[678] For present purposes, it is sufficient to say that between 2009 and 2016 (apart from the period between May 2012 and October 2013 when the control room was commanded by its own Assistant Commissioner, AC Richard Chandler) POM Hayward usually reported to AC Brown, who had a broad range of other responsibilities. It was not until the appointment of AC George as Head of Operational Response in March 2016 that the control room once again had the benefit of its own Assistant Commissioner.
In December 2015, a few months before his appointment as Assistant Commissioner and Head of Operational Response, AC George was asked by AC Brown to lead what he described as a “cultural review” of the control room and its position within the organisation.[679] In his role as Head of Operational Response, AC George was also responsible for the operation of the control room and mobilising, the operation of the Resource Management and Logistics Centre and the UK Fire and Rescue Services’ National Co-ordination Centre.[680] He was also POM Hayward’s line manager. AC George agreed that during that period POM Hayward had run the control room on a day-to-day basis, although he knew that AC George wanted to be kept informed about the type of decisions he was making.[681] AC George was also ultimately responsible for the delivery of training to CROs.[682] AC George knew that POM Hayward had delegated responsibility for training to SOM Smith and was content with that.[683] He explained that he had satisfied himself that it was an appropriate and effective step and had considered SOM Smith a very professional and experienced officer.[684] As Head of Operational Response, AC George reported directly to AC Brown.[685]
In April 2017, AC George succeeded AC Brown as Director of Operations.[686] He was not replaced as Head of Operational Response, a position that ceased to exist.[687] Although AC George retained responsibility for managing POM Hayward, he delegated all matters relating to the management of the control room to him.[688]
Following the Grenfell Tower fire, the management structure of the control room changed. In late 2018 or early 2019, AC George decided that a more senior officer needed to take over the day-to-day management of the control room.[689] POM Hayward was made redundant and Commissioner Cotton appointed AC Jonathan Smith as a new AC Operational Resilience and Control.[690] On 1 January 2021, SOM Joanne Smith was promoted to the newly created position of DAC for Control and Mobilising, reporting to AC Jonathan Smith.[691]
Control room staff held regular meetings, usually monthly, which were attended by all staff other than the CROs.[692] Although AC Chandler regularly attended those meetings, AC Brown and AC George did not.[693] AC Brown considered that, as they were meetings of middle managers, it was for the POM and SOMs to manage them.[694]
POM Hayward regarded the meetings as an opportunity to discuss matters generally and inform the watch managers about any changes in the work.[695] He also said that he would use them as a barometer to gauge whether there were any negative comments about training.[696]
For a long time, POM Hayward reported to AC Brown as his line manager. AC Brown said that he used a variety of methods to monitor the performance of the control room and the way in which it was being managed. As Director of Operations he chaired a monthly Principal Management Board meeting of the area DACs, which he encouraged POM Hayward to attend,[697] but it appears that matters relating to the control room arose only occasionally and even then represented a relatively small part of what was discussed.[698] He also met Scott Hayward once between each of those meetings, so that they met about every two weeks.[699] They also saw each other at meetings relating to one of the other areas for which AC Brown had strategic responsibility, if the subject matter affected the control room.[700]
AC Brown did not exercise any particular oversight over the training of CROs[701] because he considered that they were highly managed, in the sense that the control room contained approximately the same number of staff as a large fire station but a much higher proportion of managers.[702]
The Lakanal House fire was a particularly significant event for the control room. The Lakanal House Board identified 13 pre-inquest actions relating to the control room, the most important of which for present purposes were those concerning a review of national guidance and LFB policy on providing fire survival guidance,[703] the training of CROs and their supervisors,[704] amendments to LFB Policy No. 539 (PN539) on emergency call-handling,[705] the creation of a policy (Policy No. 790 (PN790)) on handling fire survival guidance calls,[706] and amendments to the Reference Information Files (RIFs).[707]
AC Brown was given responsibility for carrying out the pre-inquest actions,[708] a task which he delegated to POM Hayward, although he provided him with support and met him from time to time to monitor progress.[709] POM Hayward did not ask AC Brown for additional resources to carry out the work.[710]
Action 5 of the pre-inquest actions was the production of a gap analysis to identify any differences between national guidance on handling fire survival guidance calls and PN539.[711] The analysis was fundamental to shaping the control room’s response to the Lakanal House fire.
The gap analysis had been completed by April 2010. It was produced by POM Hayward in conjunction with SOM Smith, DAC Cutbill, who was leading the investigation into the Lakanal House fire, and Thomas Davies, a member of the LFB’s legal department.[712] SOM Turner, SM Hams and GM Zymanczyk also contributed to the first draft.[713] The analysis involved a comparison between two national guidance documents on the training of control room staff and the LFB’s policy on emergency call management and its training materials on fire survival guidance.[714] The report made recommendations designed to address deficiencies identified in both national guidance and LFB policy and training.[715]
Although it is not clear whether the recommendations in the gap analysis were formally approved by the Lakanal House Board, some of the gaps that had been identified and some of the resulting recommendations gave rise to further pre-inquest actions intended to address them.[716] That was certainly the case for the following recommendations:
Although the RIFs used by CROs when handling fire survival guidance calls were not specifically addressed in the gap analysis, SOM Smith said that they had used the findings of the gap analysis to revise the RIFs after the Lakanal House fire.[724]
On 8 December 2004, the government issued Fire and Rescue Service Circular 54-04 on ‘Emergency Call Management’ (FSC 54-04).[725] It provided advice and a description of good practice developed jointly by the Chief Fire Officers Association and HM Fire Service Inspectorate to assist effective emergency call-handling by fire and rescue services.[726] It was produced following a review of emergency call-handling which they had commissioned jointly in 2001.[727] One of the review’s objectives was to review existing guidance on handling emergency calls (including fire survival guidance calls).[728]
The document summarised, in the form of national guidance, a three-stage approach to handling emergency calls with the objective of improving the way in which they were managed.[729] Annex A set out a generic three-stage approach to call-handling called the “Emergency Call Management Protocol”.[730] In summary, stage 1 involved obtaining information to assist the mobilising decision,[731] stage 2 involved obtaining information to support continuous assessment and ensure the safety of everyone involved,[732] and stage 3 was directed to ensuring the safety of the caller and members of the public.[733]
Annex D contained “Fire call prompts”, which included various ‘prompts’ in relation to fire survival guidance calls to be used at stage 3 of the call-handling approach, as well as a warning that stages 1 and 2 might need to be revisited during stage 3.[734]
FSC 54-04 did not supersede FSC 10-93, so the available national guidance was to be found in a combination of the two documents.[735] Despite that, the LFB excluded FSC 54-04 from the scope of its gap analysis.[736] POM Hayward told us that FSC 54-04 had been discussed with DAC Cutbill and Thomas Davies at the time and that they had all considered that it did not need to be included[737] because it was concerned with the use of scripts, which the control room did not use at that time.[738] He also said that he did not think that FSC 54-04 added anything to the training described in FSC 10-93.[739] SOM Smith said the same.[740] AC Brown did not believe that the decision had been discussed with him and he did not recall approving it.[741]
Notwithstanding the view of PO Hayward that FSC 54-04 added nothing of substance to FSC 10-93, it is hard to reconcile the decision to exclude FSC 54-04 either with the purpose of the gap analysis or with the contents of FSC 54-04 itself. One of the stated aims of the emergency call-handling review had been to review FSC 10-93 and the training package ‘Keeping People Safe’ which the Home Office had issued to complement it. (‘Keeping People Safe’ described the training requirements for CROs and set out a recommended programme of training).[742] The express purpose of issuing FSC 54-04 had been to improve the handling of emergency calls.[743] Moreover, it was expressly intended to provide national guidance.[744] It is surprising, therefore, that it was excluded from an analysis which was specifically aimed at comparing LFB policy and training with existing national guidance. Nor was it simply about using scripts or prompts, as suggested by POM Hayward. It provided general guidance on managing emergency calls, including fire survival guidance calls.[745] Finally, and most significantly, FSC 54-04 went beyond the guidance in FSC 10-93 and ‘Keeping People Safe’ in a number of important respects. For example, it advised CROs that when taking fire survival guidance calls they should positively assess the age, gender, ethnicity and any mental and physical disability of the caller.[746] Although ‘Keeping People Safe’ referred to the possibility that a caller might be incapacitated, or unable to communicate effectively because of language difficulties or confusion, it did not encourage CROs to explore those matters as part of their assessment.[747] Further, FSC 54-04 encouraged CROs continually to assess the caller’s situation and review their initial assessment in the light of changing circumstances.[748] Neither FSC 10-93 nor ‘Keeping People Safe’ provided or reflected that guidance.[749]
FSC 54-04 should therefore have been included in the gap analysis. The fact that it had not been included was noticed in November 2012, when those drafting the Lakanal Control Report realised that the guidance in FSC 54-04 on handling fire survival guidance calls had been omitted from training materials. It was noticed again in January 2013 when GM Lindridge drew attention to it in his review of the pre-inquest actions. Yet, for no obvious reason, no action was taken to ensure that all relevant national guidance had been incorporated into LFB policy and training.
The Lakanal Control Report (dated November 2012) noted that, although some CROs handling fire survival guidance calls had tried to find out what was happening at different stages of the call, the importance of continual re-assessment had not been included in LFB training materials. Despite that finding, the Lakanal Control Report did not recommend that FSC 54-04 should be specifically referred to in the gap analysis or that a reference to the need continually to reassess the caller’s situation should be incorporated into LFB training and policy.
On 14 January 2013, DC Dexter forwarded a copy of GM Lindridge’s review to AC Brown, to which she had added her comments, and invited his response.[750] She asked why the gap analysis did not include any reference to FSC 54-04.[751] On 16 January 2013, AC Brown provided her with his response, which he said he had discussed with GM Lindridge.[752] He said that, as FSC 54-04 only partially addressed fire survival guidance calls, and then only in relation to age, gender and disability, the analysis had concentrated on the requirements of FSC 10-93. However, he said that AC Chandler had been instructed to remedy the omission in November 2013.[753]
In evidence AC Brown accepted that, because age, gender and disability were factors that might affect a caller’s ability to escape from a fire, FSC 54-04 should have formed part of the original gap analysis.[754] However, it was also important that the guidance it provided in relation to those factors be included in LFB policy and training. In those respects, AC Brown’s reply to DC Dexter understated the relevance and importance of FSC 54-04. His reply also failed to draw her attention to the guidance in FSC 54-04 that a CRO should continually reassess the caller’s situation, guidance that had been identified in the Lakanal Control Report as missing from LFB training.[755] AC Brown said he believed that he had brought it to DC Dexter’s attention during one of their regular meetings,[756] but in common with many similar assertions, we have seen no independent evidence that he did so.
AC Brown said that the purpose of his reply to DC Dexter was just to confirm that he had asked AC Chandler to consider FSC 54-04 when GM Lindridge’s review was revised.[757] AC Chandler was absent from work from late 2012 until April 2013. AC Brown said he could not remember whether AC Chandler had told him that POM Hayward would carry out the task in his absence or whether he had himself asked POM Hayward to do so,[758] but either way POM Hayward could not recall having received any such request.[759]
When he revisited his review in November 2013 and May 2014, GM Lindridge again noted that FSC 54-04 had not been included in the gap analysis. He sought to justify its omission primarily on the basis that it did not seek to provide a full account of how fire survival guidance calls should be handled.[760]
Although the exclusion of FSC 54-04 was apparently reconsidered, the gap analysis was not revised to include a comparison between LFB policy and training and FSC 54-04, despite AC Brown’s assurance to DC Dexter that the omission would be remedied. The reasons given for not doing so are clearly unsound, because the purpose of the gap analysis was to compare LFB policy and training with national guidance and the guidance in FSC 54-04 on handling fire survival guidance calls clearly went beyond that contained in FSC 10-93 and ‘Keeping People Safe’.
The failure to consider FSC 54-04 created a real risk that the guidance it contained, especially on assessing any impairments which might affect a caller’s ability to leave and on continually reassessing the caller’s situation, was not effectively reflected in LFB policy and training. As was found in the Phase 1 report, that risk materialised when PN539 was produced.[761]
The gap analysis was defective in two other significant respects: first, it failed to identify the fact that PN539 did not include the warning contained in FSC 10-93 about the dangers of offering false reassurance to a caller; secondly, despite having noted that FSC 10-93 and the LFB’s training material did not emphasise the need for continual reassessment of the caller’s situation, it failed to identify the fact that that guidance had also been omitted from PN539. We explore those defects and the likely consequences of them in relation to the revision of PN539 below.
FSC 10-93[762] and ‘Keeping People Safe’[763] both contained warnings that providing calming reassurance to callers trapped in buildings or otherwise exposed to danger could itself be dangerous. The gap analysis noted that FSC 10-93 acknowledged the possibility that an emotional bond might be formed between CROs and callers as calls progressed and emphasised that the relationship might be unhelpful because it might lead to callers’ giving answers that they think CROs want to hear. CROs were therefore advised to exercise caution when offering reassurance to avoid giving callers a false sense of security. The gap analysis also noted that the LFB’s training programme tended to encourage a strong attachment between callers and CROs by encouraging the use of reassuring phrases, which might have that effect.[764] It therefore recommended that LFB training reflect more closely the guidance in FSC 10-93 to prevent an emotional link being formed and false reassurance being given.[765]
The gap analysis did not state whether PN539 dealt with the need for caution when offering reassurance to callers and therefore did not identify a gap or make any recommendation to amend PN539 in that respect. As it was, the version of PN539 dated 14 November 2007, which was current at the time, did not include a warning similar to that found in FSC 10-93 or ‘Keeping People Safe’.[766] SOM Smith thought that that was because that guidance was to be delivered by the LFB through training rather than by policy,[767] but if that was the LFB’s position, it was unreasonable. First, it does not explain why consideration of that aspect of PN539 was entirely omitted from the gap analysis. Secondly, it does not explain why the version of PN539 dated 14 November 2007 actively encouraged CROs to provide reassurance, including by the use of phrases such as “the firefighters will be with you very soon” and “I’m going to talk to you until the firefighters arrive”, both of which might well promote a false sense of security.[768] Thirdly, it ignored, or at least underestimated, the importance of PN539’s stating clearly and fully the objectives and principles of, as well as the correct approach to, handling fire survival guidance calls. The clear and full expression of those principles would ensure that they would not be lost on anyone reading the policy (such as a CRO) and would provide a clear and comprehensive framework for training.
The failure to amend PN539 in those two respects was significant. As the chairman found in the Phase 1 report, PN539 had not been amended by the time of the Grenfell Tower fire and CROs invariably told callers that firefighters were on their way without having a sound basis for doing so.[769] As a result, some callers were lulled into a false sense of security, remained in their flats and did not attempt to leave with sufficient vigour, or at all, despite the fact that escape was possible.[770]
The gap analysis also recommended that any revision of national guidance should contain advice to CROs to reassess the situation continually in order to be aware of changing conditions in the building and the caller’s state of mind.[771] The basis for that recommendation is not entirely clear. The analysis failed to identify the fact that the current version of PN539 did not contain guidance that a CRO should continually reassess the caller’s situation,[772] so it did not include an analysis of that aspect of the policy. POM Hayward said that it had been intended to amend PN539 in that way, but he could not explain why, if that had been the case, the gap analysis had not said so.[773] That may explain why PN539 advised CROs to reassess the caller’s situation, but did not emphasise the need for continual reassessment.[774] We discuss below the reasons for the deficiencies in the version of PN539 that was current at the time of the Grenfell Tower fire.
The LFB also undertook a detailed internal review of the part that the control room had played in the LFB’s response to the fire at Lakanal House.[775] The outcome was contained in a report entitled Fire at Lakanal, Havil Street, SE5 on 3 July 2009 – Role and Actions of the LFB Control published in November 2012 (the Lakanal Control Report).[776] It was informed by the gap analysis, completed in April 2010, which had identified differences between national guidance and LFB policy and training on handling fire survival guidance calls.[777] It set out the policy framework relating to the control room, the arrangements for training of CROs, and the working practices of the control room.[778] It examined the Lakanal House fire from the perspective of the control room and identified numerous lessons.[779] The report included nine recommendations and points for further action.[780]
Of particular interest to us is the fact that the report suggested improvements to national and LFB policy on the training of CROs in handling fire survival guidance calls and managing the performance of control room staff.[781] The report identified some recommendations that had already been completed, with some subject to a continuing process of review and implementation.[782] The Lakanal Control Report was submitted to the coroner and on the basis of its contents she decided not to make any recommendations about handling fire survival guidance calls or training for CROs.[783] In her rule 43 letter she noted that the LFB had already undertaken extensive work to learn from its experience at Lakanal House.[784] The striking similarities between the failings of the control room in handling fire survival guidance calls during the Lakanal House fire and those which were later seen in its response to the Grenfell Tower fire led us to examine whether the assurances given to the coroner about policy and training relating to handling fire survival guidance calls had been properly implemented and met their objective.[785] The short answer is that they had not and did not. We shall need to return to the Lakanal Control Report more than once in this chapter.
The LFB’s policy on emergency call management is contained in Policy No. 539. Pre-inquest action 10 was to review PN539 to ensure that it complied with national guidance.[786] That was a response to the identification in the gap analysis that PN539 did not reflect current guidance, particularly the appendix on fire survival guidance calls.[787]
Responsibility for carrying out the action was assigned to AC Brown,[788] who had overall responsibility for PN539 as Head of Service Delivery & Mobilising.[789] However, he was not involved in reviewing and revising PN539, which he had delegated to POM Hayward.[790] POM Hayward, in turn, said that SOM Lindsay Turner and the Operational Support Team had carried out the task,[791] although in fact both he and SOM Smith were involved in and oversaw the work.[792]
The initial review and revision of PN539 was completed by 3 September 2010,[793] as POM Hayward and SOM Smith reported to the Lakanal House Board on 15 September 2010.[794] However, they did not present the revised version of PN539 to the board,[795] which never formally approved it.[796] Nor did AC Brown,[797] who told us that it was not normal practice for managers in his position to read through a policy and approve the changes.[798] As a result, the revisions made to PN539 after the Lakanal House fire were not subjected to any form of approval process and were not examined by the senior manager responsible for them.[799]
PN539 was amended nine more times before the Grenfell Tower fire, most significantly Appendix 3, which covered fire survival guidance calls. It was amended on 3 February 2011 and 28 March 2014.[800] The version of PN539 that was in force at the time of the fire had last been amended on 6 April 2017.[801] The Phase 1 report found that the policy was significantly defective in many respects. In particular, it failed to state clearly that the four principles of “escape, assess, protect and rescue” required continual reassessment of the caller’s situation,[802] it did not contain a warning that it is not always safe to assume that the fire and rescue service is on its way to rescue the caller,[803] it did not make it clear that, if a fire survival guidance call required a CRO to remain on the line, the number of simultaneous fire survival guidance calls could never exceed the number of CROs available,[804] it contained no advice or guidance to assist CROs and senior managers when handling a large number of fire survival guidance calls concurrently[805] and it did not require CROs to find out whether the caller was, or had with them, a person who, for whatever reason, would require help to evacuate.[806] We explore the reasons for those defects below.
The exclusion of FSC 54-04 from the gap analysis created a risk that the guidance it contained on the need continually to reassess the caller’s situation would not be reflected in PN539. Curiously, however, the version of PN539 dated 3 September 2010, which was the result of the first revision following the Lakanal House fire, did add advice to CROs to reassess continually the caller’s situation,[807] but it was replaced in the version dated 3 February 2011 with advice to reassess the caller’s situation, providing some example questions.[808] The clear and unambiguous emphasis on continual reassessment had thus been removed and the policy remained in that form until the Grenfell Tower fire.[809]
It is evident from the version of PN539 that SOM Smith sent to POM Hayward on 3 February 2011 with tracked changes that she was the person who removed the requirement for continual reassessment.[810] When asked, she could not account for that,[811] but she suggested that the amendments amounted to the same thing and that the training made that clear.[812] She told us that the need for continual reassessment, although not stated explicitly, was implied in the revised version[813] and that training emphasised the need for continual reassessment.[814] AC Brown said essentially the same.[815] However, those explanations ignored, or at least underestimated, the vital importance of ensuring that PN539 stated clearly and comprehensively the objectives, principles and approach for handling fire survival guidance calls.
As set out above, the Lakanal Control Report, dated November 2012, which post-dated the removal by SOM Smith of the passage emphasising the need for continual re-assessment, found that the guidance in FSC 54-04 was not included in LFB training and that there might be a tendency among CROs to limit reassessment due to a desire to keep the caller safe.[816] It recommended that PN539 should be revised to ensure compliance with national guidance and to reflect the lessons identified in the report.[817] However, it also recorded that PN539 had already been revised in February 2011,[818] implying that no further action was required. There is nothing to suggest that the recommendation prompted any further consideration of PN539 to ensure that it reflected in full the experience of the Lakanal House fire. AC Brown confirmed that he had not asked for any further work to be done on it.[819]
In his review dated 4 January 2013, GM Lindridge found that PN539 did not incorporate the guidance in FSC 54-04,[820] a conclusion which he said had been reported to AC Brown as AC Operations, Prevention and Response. GM Lindridge understood that his observations would be considered in a forthcoming review of policy on handling fire survival guidance calls,[821] but no such review was undertaken, as AC Brown confirmed.[822] AC Brown said that he had asked AC Chandler and then POM Hayward, in AC Chandler’s absence, to review the gap analysis in relation to FSC 54-04 and to apply any resulting recommendations,[823] but that was not done and no good explanation was given for the omission.
Those were yet more missed opportunities to ensure that PN539 contained the important requirement for continual reassessment.
The version of PN539 dated 3 September 2010, which was the result of the initial revision following the Lakanal House fire, actively encouraged CROs to offer callers reassurance,[824] suggesting the use of phrases such as “the firefighters will be with you very soon” and “the firefighters know where you are”.[825] It also referred the CROs to the RIFs to assist them in providing reassurance to the caller that help was on its way.[826] However, the version dated 3 February 2011 largely removed that guidance, apart from the reference to the RIFs.[827] It simply included advice to reassure the caller.[828] It would seem that those carrying out the review of PN539 in 2011 had in mind, to an extent, the guidance in FSC 10-93 and ‘Keeping People Safe’. SOM Smith confirmed as much when she said that the emphasis on reassurance had been removed because of the warning in FSC 10-93 and the investigation into the Lakanal House fire.[829]
In those circumstances, it is hard to understand why those who updated PN539 in February 2011, a group which included SOM Smith and POM Hayward, did not include an explicit warning to CROs, as set out in the national guidance, against providing reassurance to callers which might promote a false sense of security.[830]
SOM Smith said that training had included clearer instructions on the warning and there might also have been advice in the RIFs.[831] That was certainly not so in the case of the RIFs, as the chairman found in the Phase 1 report. In any event, it ignored or, at least, underestimated the important role of the policy and placed too much reliance on training.[832]
The Lakanal Control Report dated November 2012 noted that CROs handling fire survival guidance calls during the Lakanal House fire expected fire crews to arrive quickly (as they usually did) and advised callers to remain in their flats and wait to be rescued rather than helping them to assess whether escape was possible.[833] The implication was that an assumption that firefighters would rescue a caller promptly, or at all, was not always well founded. That echoed the warning in FSC 10-93 and ‘Keeping People Safe’ against providing reassurance to a caller which might produce a false sense of security.[834] However, despite the recommendation in the Lakanal Control Report, that aspect of PN539 was not reconsidered and the policy was not amended to include an appropriate warning.
Further, in his review dated 4 January 2013, GM Lindridge found that PN539 had been reviewed and did not contradict FSC 10-93, but that it might be said not to contain all the information in the national guidance.[835] In a comment on the draft DC Dexter asked whether PN539 complied with national guidance, to which AC Brown replied that it did and that the action had been completed, both in word and spirit,[836] but that was wrong because PN539 did not include a warning against providing false reassurance.[837] It appears that, as a result, no action was taken to investigate and deal with this particular aspect of GM Lindridge’s review.
The failure to include FSC 54-04 in the gap analysis created a real risk that the guidance it contained about assessing any impairments which might impede a caller’s ability to escape would not be reflected in LFB policy and training. In fact, the version of PN539 dated 14 November 2007 did include a requirement for CROs to assess whether callers had any relevant disabilities,[838] but for no obvious reason that requirement was removed from later versions and was not reinstated before the Grenfell Tower fire.[839] SOM Smith could not explain why.[840] She told us that she had not been involved in the revision of PN539 in 2010,[841] but email exchanges at the time reveal that she, together with POM Hayward, SOM Turner and Amelia Reynolds, had all contributed to it.[842] SOM Smith said that she was not aware of any positive decision to omit the advice on assessing disability[843] and could not say whether it had been omitted accidentally.[844] She said that she had made sure that the questions on disability were included in the training and the RIFs,[845] but that was not the case as far as the RIFs were concerned.
The RIF for Operators dated 12 March 2007 had contained a prompt to ask whether a caller had a disability and whether their mobility was impaired, but that prompt was removed from the revised version approved by SOM Smith on 23 February 2011.[846] However, unlike PN539, a later version of the RIF for Operators approved by SOM Bagnelle on 3 April 2014 reinstated a prompt that did effectively address the requirement to assess disability, albeit with rather less emphasis than previously.[847]
SOM Smith’s evidence was that she had thought that the reason why the requirement to assess disability had not been reinstated in PN539 in February 2011 and thereafter was because it had been covered by training and in the RIFs and it was felt that that was sufficient.[848] However, the RIFs were not amended until April 2014 and we do not consider that training could adequately compensate for its omission from the policy, since that leaves too much to the discretion of the individual trainer. SOM Smith told us that it was not unusual for a CRO to assess the caller’s age and ability to leave the building,[849] She effectively accepted that much depended on what information the caller provided.[850] If so, that was not consistent with national guidance, because FSC 54-04 clearly required CROs to carry out a positive assessment of a caller’s age, gender, ethnicity and mental or physical disability.[851] SOM Smith accepted that the LFB was not following the guidance in FSC 54-04;[852] she also accepted that, if it were left to the caller to volunteer information, there was a risk that it might not be given, which is exactly what happened in some cases during the Grenfell Tower fire.[853]
In his review dated 4 January 2013 GM Lindridge found that PN539 did not include the guidance called for by FSC 54-04.[854] That omission might, therefore, have been made good if some action had been taken in response to his finding. However, it was not.
A further opportunity to remedy the omission came in the form of GRA 3.2, published in February 2014,[855] which introduced new requirements for handling fire survival guidance calls.[856] AC Brown was involved in the consultation process which preceded the document.[857] However, it is reasonably clear that he did not discuss it with anyone else responsible for the operation of the control room.
GRA 3.2 introduced a requirement for fire and rescue authorities to have effective arrangements in place for handling fire survival guidance calls from those who believe they are unable to leave a building due to disability, poor mobility, illness or the effects of fire. However, AC Brown admitted that he had taken no specific steps following the publication of GRA 3.2 to ensure that the LFB had such arrangements in place because he was satisfied that CROs would obtain that information and that adequate arrangements were therefore already in place.[858] He had not considered asking anyone responsible for the control room to review PN539 to ensure that it was consistent with GRA 3.2.[859] Unsurprisingly, in the light of their ignorance of GRA 3.2, POM Hayward and SOM Smith did not carry out any such review themselves, nor did POM Hayward ask anyone else to do so.[860]
The direct result of this cluster of failings was that the LFB did not introduce, or reintroduce, into PN539 a provision for CROs to enquire positively whether callers had disabilities or other impairments of a kind that might affect their ability to leave the building.
A further, and perhaps final, opportunity to remedy that particular deficiency was by way of an equality impact assessment, which ought to have been undertaken in order to consider the likely effect of the policy on different groups of people. However, it is evident from the audit trail in the version of PN539 which was current at the time of the Grenfell Tower fire that no one carried out such an assessment after 17 September 2008.[861]
AC Brown accepted that it had been his responsibility to ensure that an equality impact assessment was carried out,[862] but he said that such an assessment was carried out only when changes were made that required one.[863] He did not think that they had decided it was necessary to carry out an equality impact assessment when PN539 had subsequently been reviewed after 2008.[864] However, he acknowledged that in hindsight one should probably have been carried out at some point.[865]
In our view, the warning signs were there at the time for all to see. AC Brown simply did not heed them. It is surprising that he took no steps to alert the LFB’s senior management to the existence, let alone the contents, of GRA 3.2 or to recognise the need for an equality impact assessment. We regard those as serious failings on his part.
Pre-inquest action 9 was to revise the Reference Information Files (RIFs) used by CROs when giving fire survival guidance in order to ensure that they complied with national guidance.[866] There were two RIFs: a RIF for Operators, which was a prompt sheet or script to assist with handling fire survival guidance calls, and a RIF for Supervisors, which described their role in supporting CROs during fire survival guidance calls and passing information to the incident ground.[867]
SOM Turner, SOM Smith and the Operational Support Team carried out the revisions to the RIFs in discussion with POM Hayward.[868] SOM Turner undertook the initial review;[869] SOM Smith then proposed further revisions.[870] They were completed by January 2011 and circulated to control room staff on 23 February 2011.[871]
SOM Smith said that the primary reason for revising the RIFs following the Lakanal House fire was to prepare for the next large-scale incident.[872] Senior management wanted to ensure that the RIFs contained clear advice in relation to fires in high-rise residential buildings.[873] The RIF for Operators was, therefore, amended so that there were sections on different types of buildings, with a separate section on purpose-built blocks of flats.[874] SOM Smith said that she had also used the findings of the gap analysis to amend the RIFs.[875]
SOM Smith approved the revisions to the RIFs.[876] Although she discussed some of them with POM Hayward, it is reasonably clear that he did not review or approve the revisions, even though responsibility for final approval lay with him.[877] Further, although POM Hayward and SOM Smith informed the Lakanal House Board on 15 September 2010 and 4 February 2011 of the fact that the RIFs had been revised, they did not describe the substance of the revisions.[878] As a result, the Lakanal House Board did not formally review and approve the changes.
On 27 June 2011, AOM Bonnett sent an email to SOM Smith, SOM Turner, AOM Sharp and AOM O’Shea in which he criticised the training relating to fire survival guidance as being inconsistent with the revised RIF for Operators.[879] He concluded that, because the RIF had been specifically designed to assist CROs during fire survival guidance calls, it should be central to, and consistent with, training.[880] He also suggested that training exercises should be carried out to test the suitability of both the RIF for Operators and the RIF for Supervisors.[881]
SOM Smith forwarded the email to POM Hayward, expressing her agreement with AOM Bonnett’s findings.[882] Despite her agreement, however, no training was provided on the RIFs, nor were they subject to a test exercise.[883] Control room staff were simply notified that the RIFs had been revised and told to familiarise themselves with their contents.[884] SOM Smith said that was because staff could look at the RIFs at any time they wished and because, contrary to AOM Bonnett’s opinion, they were consistent with the fire survival guidance training.[885]
We do not understand how senior management could have satisfied themselves that CROs and supervisors understood the nature and extent of the changes to the RIFs that had been brought about as a consequence of the Lakanal House fire without providing them with any formal training. As it was, the training records we have seen show that no staff reviewed the RIFs in 2011 and that only two did so in 2012.[886]
The RIFs were revised again in early 2013 following discussions with GM Lindridge.[887] SOM Vic Bagnelle instructed AOM Bonnett and AOM Pope of the Operational Support Team to carry out the revisions, which he then reviewed and approved on 18 February 2013.[888] The primary aim of those revisions was to reduce the length of the RIFs to make them more manageable.[889] As a result, the separate sections on different building types, including purpose-built blocks of flats, were removed.[890]
Although SOM Bagnelle reported to POM Hayward and AC Brown on the progress of their work, we have not seen any evidence that POM Hayward or the Lakanal House Board reviewed or approved the revised versions.[891]
AOM Bonnett circulated the revised RIFs to control room staff on 18 February 2013.[892] As before, they were simply instructed to familiarise themselves with the contents.[893] The training records indicate, however, that most staff did not review the RIFs in 2013 and there are no records of any staff having done so thereafter.[894]
SOM Sharp made further amendments to the RIFs in 2014, which were approved by SOM Victor Bagnelle on 3 April 2014.[895] That then remained the version of the RIF for Operators in force at the time of the Grenfell Tower fire.[896] The RIF for Supervisors, however, was revised once more before the Grenfell Tower fire in April 2016, although the revisions do not appear to have been formally approved.[897] The version in force at the time of the Grenfell Tower fire had, therefore, been approved on 3 April 2014 and subsequently amended on 2 April 2016.[898]
In his Phase 1 report the chairman found that the RIF for Operators was unsatisfactory in a number of respects.[899] It contained no clear guidance on what was meant by “affected” by heat, smoke or fire or how it was to be assessed, it contained no clear guidance on how to assess the safety of escape routes if the caller was, or claimed to be, affected by heat, smoke or fire, or simply felt unsafe, it did not tell CROs that assurances that firefighters would rescue callers should be based on information from the incident ground rather than expectations or assumptions, it contained no guidance on what information CROs should gather in order to assist the control room supervisor or incident commander to decide whether a partial or total evacuation of the building should be carried out and it contained no guidance on what advice CROs should give to a caller once a decision had been made to carry out a full or partial evacuation of the building. He also found that the RIF for Supervisors contained similar defects. In particular, it contained no guidance on how supervisors should gather information from CROs to enable them to form an overall assessment of the situation in order to assist incident commanders to decide whether to revoke “stay put” advice.[900] We consider the reasons for those defects below.
The section of the RIF for Operators dated 23 February 2011 that dealt with giving fire survival guidance to a person trapped in a purpose-built flat, advised the CRO to ask the caller whether the flat was being “affected” by heat or smoke. If the caller said it was not, the advice was to say that it would usually be safer to stay in the flat, but that if the situation changed, or the caller felt unsafe, the better course was to get out and stay out.[901]
SOM Smith had been responsible for drafting that advice.[902] She said that she had taken the word “affected” from FSC 10-93, although that word is not used in the circular.[903] She understood it to mean that heat or smoke was entering the flat and directly affecting the caller in some way, such as interfering with their breathing;[904] in effect, that compartmentation had been breached.[905] When preparing the RIFs, SOM Smith had asked John Bradbury, DAC Fire Safety Regulation Delivery, and AC James Knighton, AC Operational Policy, what information it would be helpful to obtain from a caller to enable a CRO to determine whether the person was affected by fire, heat or smoke,[906] but they had not given her any help.[907] However, despite her own understanding and her difficulty in obtaining assistance, she did not consider including in the RIF an explanation of what “affected” meant or further prompts to guide a CRO when giving advice.[908]
The RIF for Operators also suggested that, if a caller was, or felt themselves to be, “affected” by fire, heat or smoke, CROs should ask about possible escape routes.[909] It then set out questions aimed at finding out whether an alternative escape route was available.[910] However, the RIF did not suggest how to assess the safety of any potential escape route. SOM Smith said that when she drafted the RIF she must, at some point, have considered whether such guidance was needed, given the questions on exploring alternative escape routes that she had included.[911] If so, it must follow that she decided not to include such guidance.
The revised versions of the RIFs for Operators dated 18 February 2013 and 3 April 2014 contained the same defects.[912] The revision in 2013 concentrated principally on reducing its length and making it easier to use rather than on making substantive changes.[913] It is not surprising, therefore, that SOM Bagnelle and SOM Sharp do not appear to have considered providing guidance on the meaning of being “affected” by fire, heat or smoke or on assessing the safety of an escape route. However, SOM Bagnelle said that the amendments made in April 2014 had included additional questions for CROs to use following comments made by command unit staff during training workshops[914] to the effect that finding out how far the caller’s flat was from the nearest stairwell would help a CRO decide whether the caller could reach it.[915] It was suggested that a conversation of that kind might cause the caller to consider the layout of the property and realise that escape was possible[916] and that a prompt might be included in the RIF to that effect.[917]
Despite that, when they revised the RIF for Operators in April 2014 neither SOM Sharp nor SOM Bagnelle included a prompt of that kind.[918] Moreover, it is reasonably clear that the comments from the workshops did not cause either of them to consider whether guidance on assessing the safety of escape routes, beyond the distance to the stairwell, should be included.
The failure to include such guidance was significant because, as the chairman found in the Phase 1 report, CROs failed properly to assess escape routes on the night of the Grenfell Tower fire and advised callers to stay put, even though they may not in fact have been trapped, with the result that some callers may have stayed in their flats when they could have escaped to safety.[919]
The gap analysis drew attention to the warnings in both FSC 10-93 and ‘Keeping People Safe’ about forming an emotional bond with a caller and providing false reassurance.[920] It identified that the training of CROs encouraged the creation of a strong attachment between the caller and the CRO and that it recommended using reassuring phrases that might promote a false sense of security.[921] Accordingly, the gap analysis recommended that training be changed in those respects.[922]
SOM Smith used the findings of the gap analysis to revise the RIFs,[923] but despite that, the revised RIF for Operators she approved on 23 February 2011, like PN539, actively encouraged CROs to reassure the caller.[924] It suggested the use of phrases such as “the firefighters are on the way” and “the firefighters know where you are”.[925] However, the RIF included no warning to the CROs against providing false reassurance nor did it make it clear that such statements must be made only if based on information received from the incident ground.[926]
On 3 January 2011, SOM Smith had emailed AOM Bonnett and AOM Suarez with a draft of the revised RIF for Operators.[927] Anticipating the concerns of the Lakanal House Board that it did not appear in national guidance, she had removed the word “bonding”.[928] It is evident, therefore, that SOM Smith had the gap analysis and national guidance in mind when she was revising the RIF.[929] In those circumstances, it is hard to understand why she did not include the explicit warning against providing a false sense of security or why she felt it was sufficient to remove only the word “bonding” from the RIF and not the associated statements which had been designed to reassure and create a bond with the caller.[930]
SOM Smith said she had not included a warning against providing false reassurance because it was guidance on what should be done rather than what should not be done, so it had not occurred to her or the Operational Support Team to include it.[931] Even if that were right, however, it presented no bar to including positive guidance in the RIF that a CRO should provide reassurance to callers only if it were based on information received from the incident ground. The suggestion by SOM Smith that it was a matter covered in training[932] placed too much reliance on training and ignored, or at least underestimated, the importance of ensuring that the RIFs stated accurately and comprehensively the correct approach to handling fire survival guidance calls in accordance with national guidance.
The work on revising the RIFs should have included a comparison with the guidance contained in FSC 10-93 and ‘Keeping People Safe’ in order to ensure that they were compatible and that nothing had been omitted. However, that was not done and all the later versions of the RIFs suffered from the same defect.[933] Again, that was significant because CROs invariably told callers on the night of the Grenfell Tower fire that firefighters were on their way without having a sound basis for doing so. The tragic result was that some callers remained in their flats despite the fact that escape may have remained possible.[934]
SOM Smith and SM Utting were together responsible for drafting PN155 (which later became PN790), the policy on fire survival guidance calls.[935] The draft version of PN155 dated 10 February 2011 included a warning that in exceptional circumstances the incident commander might tell the control room to advise callers seeking fire survival guidance to do their best to leave their properties.[936] SOM Smith said that she had recommended the inclusion of that paragraph, although she had not been responsible for drafting it.[937] The wording suggests that the incident commander was responsible for any decision to revoke “stay put” advice. SOM Smith, however, said that she had it in mind that the decision would be made jointly by the control room and the incident commander.[938] Indeed, in its final form PN790 stated that the decision would be made by agreement between the incident commander and the officer in charge of the control room.[939]
SOM Smith does not appear to have given any thought to what might constitute “exceptional circumstances” sufficient to justify the revocation of “stay put” advice.[940] Nor did she consider providing guidance, whether to the CROs handling fire survival guidance calls or those supervising them, on what information to look out for or gather in order to help decide whether exceptional circumstances requiring an evacuation existed.[941] Nor, it appears, did POM Hayward,[942] with the result that no such guidance was included in the RIFs.
Perhaps more importantly, SOM Smith did not consider including in the RIFs guidance about what a CRO should tell a caller if the decision had been made to revoke the “stay put” advice.[943] SOM Smith said that had been because the advice would differ depending on the particular circumstances, so that, in effect, it could not be the subject of generic guidance.[944] However, she also said that they did not think that such extreme circumstances were likely to occur.[945] POM Hayward said much the same,[946] but their position makes little sense, given that the policy specifically envisaged that the “stay put” advice might need to be revoked. It is also regrettable, given what was said about it in GRA 3.2,[947] which AC Brown unfortunately failed to pass on to POM Hayward or SOM Smith.
On 13 April 2011, a draft of PN155 was sent to all Assistant Commissioners, including AC Brown, with a request that they assess its effect on their respective departments.[948] AC Brown thought that CROs would need guidance on the implementation of the provision relating to the revocation of “stay put” advice,[949] in the form of policy, RIFs and training, but he did not consider what form that guidance should take.[950] He assumed that those working on the policy and the RIFs would do that, but it is clear, not least from the absence of any guidance, that he did not take steps to ensure that it was done.[951]
The failure to include guidance of that kind in the RIFs was significant because, as the chairman found in the Phase 1 report, on the night of the Grenfell Tower fire SOM Smith and DAC Fenton had to make the difficult decision to revoke the “stay put” advice without the benefit of any established guidance. Moreover, many CROs struggled to deliver clear advice to callers that they must leave the building.[952]
Pre-inquest action 13 was to draft a letter to DCLG seeking clarification of the national guidance on handling fire survival guidance calls in order to ensure a consistent approach among fire and rescue services.[953] The letter was also intended to recommend a review of national guidance on the subject.[954]
By April 2010 POM Hayward and SOM Smith had produced a draft letter to DCLG.[955] However, on 20 April 2011 the Lakanal House Board decided not to pursue the matter until the Lakanal Control Report had been completed.[956] Notwithstanding that decision, on 20 November 2011, after the letter had been reviewed by the LFB legal team, POM Hayward asked for it to be sent to DCLG.[957] On 12 December 2011, Commissioner Dobson confirmed that it should be sent and asked for a copy to sign.[958]
On 3 February 2012, a draft of the letter dated 23 December 2011 was sent by Linda Armstrong, Deputy Head of Legal Service, by email to Sue Marshall, Commissioner Dobson’s secretary, for final approval and signature by the Commissioner with a request that it be addressed to Sir Ken Knight, then Chief Fire and Rescue Adviser.[959] There is another version of the letter dated 3 February 2012 addressed to Sir Ken Knight.[960]
The letter suggested that the relationship between FSC 10-93 and FSC 54-04 should be reviewed and that in any review of the provision of fire survival guidance there were seven areas to which particular consideration should be given. They included better guidance on engaging with callers when assessing their situation and exploring possible means of protection and escape, continual reassessment of changing conditions and the caller’s physical and mental condition, guidance on effective communications between the control room and the incident ground and training on the role of supervisors in the control room.[961]
SOM Smith said that she had felt that national guidance needed to be revised in that way because of the LFB’s experience at the Lakanal House fire and because a lot had changed since FSC 10-93 had been published.[962] She had felt that it was necessary that someone with that degree of experience should investigate whether there were new practices that could help control room staff.[963] She had assumed that other fire and rescue services might make the same mistakes as the LFB had made at the Lakanal House fire and would benefit from what the LFB had learnt.[964]
Despite SOM Smith’s view and the decision in December 2011 to send the letter to DCLG, it was not in fact sent. A later decision was made in July 2012, apparently by DC Dexter, to defer once again sending the letter until work on the Lakanal Control Report had been completed.[965]
The version of the Lakanal Control Report dated November 2012 was unequivocal in recommending that Commissioner Dobson should write to DCLG to prompt a review of national guidance on handling fire survival guidance calls.[966] However, despite that recommendation, Commissioner Dobson decided on 19 November 2012 not to send the letter.[967] His decision was reconsidered at the meeting of the board on 14 December 2012, however, when he decided that it would be reviewed after the conclusion of the Lakanal House inquests.[968] Commissioner Dobson thought that decision had been discussed at the Lakanal House Board.[969] He said that he had been persuaded that it was better to wait for the coroner’s conclusions.[970] However, in September 2013, he decided that the letter was no longer required and had been dealt with by the outcomes of the inquest.[971] He said that he had taken that decision on the advice of the Lakanal House Board.[972]
However, the coroner’s rule 43 letters did not deal with the matters raised in the draft letter to the DCLG,[973] so it is not clear why Commissioner Dobson thought that the matters it raised had been dealt with by the outcome of the inquests. The consequence of the decision not to send the letter in September 2013 was that, almost three and half years after the pre-inquest action had been raised and the letter to DCLG had been drafted, it had still not been sent. As a result, the respects in which national guidance on the handling of fire survival guidance calls needed to be improved were not considered by DCLG. It also meant that the recommendation in the Lakanal Control Report was not carried out. The coroner was not informed of that, an omission which Commissioner Dobson described as an oversight.[974]
In his review dated 4 January 2013 GM Lindridge found that the gap analysis had identified areas in which national guidance could be improved which had not been incorporated into LFB policy.[975] DC Dexter asked why that had not been done. AC Brown said that all the suggestions had been adopted where relevant.[976] However, AC Brown’s confidence was misplaced because not all GM Lindridge’s recommendations for improvement in national guidance had been considered and adopted. In particular, the gap analysis had recommended that national guidance be improved to emphasise the need for continual reassessment of the caller’s circumstances,[977] but PN539 did not emphasise that, although AC Brown thought it was implicit.[978]
AC Brown said that when AC Chandler had returned to work he had asked him to review the audit and satisfy himself that everything had been done.[979] It is clear, however, from the terms of AC Brown’s instructions that he did not ask AC Chandler to check whether all the recommendations to improve national guidance had been covered by LFB policy.[980] It is equally clear that AC Chandler did not deal with it in his response.[981] POM Hayward could not recall whether any other action had been taken in response to the recommendation.[982]
We have come to the conclusion that no action was taken in response to that particular recommendation and that as a result, an opportunity was missed to correct some of the defects in PN539, including the absence of the important emphasis on the need for continual reassessment of the caller’s situation.
In the Phase 1 report the chairman identified the need to examine whether, when, and to what extent the LFB was aware of the deficiencies that existed in its policy and training for fires that gave rise to a large number of concurrent fire survival guidance calls.[983] He found that PN539 was defective, in part because it did not recognise the important fact that, because a fire survival guidance call (as defined) requires the continued presence of a CRO on the line, the number of calls that could be handled concurrently could not exceed the number of CROs available.[984]
The definition of a fire survival guidance call in PN539 was introduced after the Lakanal House fire because the LFB had wanted something more robust than had previously existed.[985] It was formulated by those working in the control room, together with DACs Tim Cutbill and Tom Davies, and was agreed by the Lakanal House Board.[986] It did not come from national guidance.[987] SOM Smith said that people had realised at the time that the number of simultaneous fire survival guidance calls could not exceed the number of CROs and supervisors available, but that in the past the control room had never received more fire survival guidance calls than it could handle.[988]
In PN539 a fire survival guidance call is defined as
“a call to Brigade Control where the caller believes that they are unable to leave their premises due to the effects of fire, and where the Control Room Officer remains on the line providing appropriate advice until either the caller is able to leave by their own means, is rescued by the Fire brigade or the line is cleared”.
It became apparent during the evidence, particularly that of SOM Smith, that the definition is open to different interpretations,[989] since it depends on an exercise of judgement by the relevant CRO about the content of the call.[990] As a result, the precise number of fire survival guidance calls reported at any one incident could itself be a matter of debate.[991] For example, evidence about the Marriott Hotel fire on 11 November 2010, a ten-pump fire in a hotel and private residential block of 32 floors in Poplar, East London,[992] variously suggested that the control room had received between four and seventeen fire survival guidance calls.[993] The LFB’s contemporaneous documentary evidence from the Adair Tower fire on 31 October 2015, an eight-pump fire in a high-rise residential block of flats located in the Royal Borough of Kensington and Chelsea, suggested that nine fire survival guidance calls had been received,[994] but SOM Smith told us that when she had listened to the calls before giving evidence, she had reached the conclusion that only six could properly be described as fire survival guidance calls.[995]
It is difficult to understand how the identification of a fire survival guidance call could have remained a source of debate within the LFB after the Lakanal House fire, particularly when handling three fire survival guidance calls concurrently was a complex and intense experience. If the LFB could not consistently and accurately identify a fire survival guidance call, it could not tell how many had been generated by any particular incident, making it impossible to draw reliable conclusions or plan for future incidents. We have therefore sought to examine what lessons for handling fire survival guidance calls the LFB learned from the Lakanal House fire, which gave rise to five fire survival guidance calls, three of which were being dealt with at the same time.[996]
Before the Grenfell Tower fire, there had been a consensus among senior managers that the Lakanal House fire had been an exceptional event and that under normal circumstances the control room was unlikely to receive more than two or three fire survival guidance calls from any incident.[997] Although SOM Smith initially said that the expression “multiple fire survival guidance calls” was not used within the LFB or nationally,[998] it is clear that the LFB had made preparations for the receipt of two simultaneous calls, which could be viewed as “multiple” fire survival guidance calls.[999]
One striking aspect of the senior managers’ evidence was their common belief that the control room’s experience with the Lakanal House fire would not be repeated and that it was highly unlikely that more than three fire survival guidance calls would ever be received during one incident.[1000] That belief should have been questioned following a number of major fires attended by the LFB which involved a significant number of fire survival guidance calls, and certainly more than two or three.
The first such incident was the fire at the Marriott Hotel in Poplar, London, on 11 November 2010.[1001] SOM Smith was in attendance that night as control duty manager.[1002] On that occasion the control room received between four and seventeen fire survival guidance calls (depending on how one defines them) during the course of the incident, which led to seven or eight messages being passed to the incident ground about persons trapped in their flats.[1003] SOM Smith thought that there had been two concurrent fire survival guidance calls which had lasted for 45 minutes and one hour respectively.[1004] After the incident, AC Hickmott sent an email to Commissioner Dobson, Deputy Commissioner Dexter, AC Cowup, AC Brown and POM Hayward, in which he described the particularly challenging nature of many of the fire survival guidance calls, some of which had lasted for more than an hour.[1005] By contrast, AC Brown saw the incident as little more than a normal, if busy, day,[1006] a remark which we consider revealed a degree of insouciance about the magnitude of the problem.
Although the incident generated more fire survival guidance calls than the Lakanal House fire, their number did not prompt any discussion about the control room’s capacity to handle multiple fire survival guidance calls.[1007] According to AC Brown, that was because the control room had handled them very well.[1008] Be that as it may, it did not prompt any consideration of the need to plan or train for an incident which generated eight simultaneous fire survival guidance calls.[1009] According to AC Brown that was because the LFB was already taking the steps identified in the Lakanal Control report by developing PN790 and had started giving training on handling fire survival guidance calls.[1010]
On 16 June 2011, the LFB carried out an eight-pump exercise called the Heygate Challenge.[1011] It was developed to test the proposed amendments to the high-rise firefighting policy and the new draft policy on fire survival guidance calls.[1012] POM Hayward and SOM Smith representing the control room were involved as observers and facilitators.[1013] As part of the exercise the control room simulated a live incident, allocating specific pumps and passing information from mock fire survival guidance calls to the incident ground.[1014] The exercise included four fire survival guidance calls, although it is unclear whether they were concurrent.[1015] It is unclear why only four fire survival guidance calls were chosen, given that five calls had been received at the Lakanal House fire.[1016]
After the exercise, a debriefing meeting was held.[1017] SOM Smith could not recall attending it or being involved in any discussion or meeting after the exercise.[1018] Although POM Hayward thought that he had attended the meeting, the minutes do not record any contribution from the control room.[1019] Later reports from the command units recorded a consensus that the form used by staff in the command units had worked adequately for four flats as simulated in the exercise, but that the process would have been unmanageable for 20 or more calls, as one command unit had experienced at a previous incident.[1020] Further analysis noted that recording fire survival guidance calls was hard enough with four flats involved, but would be almost impossible if 60 flats were involved.[1021]
Although the Heygate Challenge involved only four fire survival guidance calls, the reports on that exercise show that the LFB was aware that multiple fire survival calls could arise from a single incident and that in those circumstances an efficient flow of information to the command units could not be maintained. Despite that, no attempt was made to plan for an incident that could generate as many as 60 fire survival guidance calls,[1022] probably because the LFB had never experienced an incident involving 60 flats.[1023] At all events, it seems clear that there was no discussion among those responsible for the operation of the control room about how it would handle more than four concurrent fire survival guidance calls. It is also clear that by mid-2011 a picture was developing that showed that incidents could give rise to more (and conceivably many more) than two or three calls of that kind.
As we noted earlier, during 2011, PN155 was being drafted predominantly by SM Utting and SOM Joanne Smith.[1024] Paragraph 7.10 of one draft specifically contemplated that the control room might receive multiple fire survival guidance calls, because it suggested that the incident commander should consider calling for an additional command unit to help managing a large number of such calls .[1025] However, there was no consensus between SM Utting and SOM Smith, or indeed between other senior managers of the LFB, on what a large number of fire survival guidance calls might mean or about how many fire survival guidance calls might be generated by any one incident.[1026] It is unclear why no consensus had been reached on that, given that the policy was specifically directed to handling multiple fire survival guidance calls, or why officers had up to five calls in mind when it had already become apparent from the Marriott hotel fire and the Heygate Challenge that it was possible for a single incident to generate many more calls.
In February 2014, GRA 3.2 was published.[1027] It included a section entitled “Fire Survival Guidance” which emphasised that numerous fire survival guidance calls could be received during a single high-rise incident.[1028] The guidance was relevant to the control room’s ability to handle numerous fire survival guidance calls, but none of those responsible for its operation appears to have been asked to review GRA 3.2 or even to have been consulted about its contents. Although it contained advice on handling fire survival guidance calls, neither POM Hayward nor SOM Smith had been aware of it before the Inquiry brought it to their attention because of its focus on operational matters.[1029] The result was that there was no discussion about how the control room would handle multiple fire survival guidance calls as GRA 3.2 contemplated.[1030]
During Phase 1 the chairman heard evidence about a tactical decision exercise training programme involving seven fire survival guidance calls that SM Peter Johnson had devised in 2014. Its purpose was to ascertain the maximum number of fire survival guidance calls that the control room and incident ground could handle satisfactorily at any one time. He also expected it to demonstrate that the procedures for handling fire survival guidance calls were inadequate.[1031] In Phase 2, we have investigated why the LFB did not proceed with SM Johnson’s programme. His exercise was sent to borough commander Terence Harrington on 27 February 2014 and presented to the fire survival guidance policy group on 12 March 2014.[1032] At that time, GM Harrington was trying to develop a practical exercise involving the structured delivery of training to impart knowledge, clarify roles and responsibilities and better understand the complexities of handling fire survival guidance calls arising from a small-scale incident that escalates to something larger.[1033] He decided that SM Johnson’s training programme did not meet that aim and it was therefore not implemented.[1034] However, even though SM Johnson’s proposal was not taken any further, it demonstrates that there was some recognition in 2014 that more than four or five concurrent fire survival guidance calls might arise from a single incident, that the systems might not be capable of managing them and that preparations should be made to deal with them. Unfortunately, that view was neither shared nor discussed more widely within the LFB.[1035]
The last significant incident before the Grenfell Tower fire which gave rise to fire survival guidance calls was an eight-pump fire at Adair Tower on 31 October 2015.[1036] Between six and nine fire survival guidance calls were received between 08.54 and 09.08, together with 15 other calls.[1037] The incident made it clear that the control room could receive more than two or three fire survival guidance calls during a single high-rise fire. Although SOM Smith described the incident as manageable,[1038] she was able to shed little light on why senior officers continued to believe that a single incident would be unlikely to give rise to more than two or three fire survival guidance calls and that more than five such calls was unthinkable.
Even though the control room had received an exceptional number of fire survival guidance calls during the Adair Tower fire, the incident did not prompt any consideration of how so many calls should be managed.[1039] It was not just the number of calls that should have prompted a review. A novel practice of recording information relating to calls on a whiteboard, which was not provided for in policy, was adopted at that incident.[1040] More importantly, most of the calls were taken by CROs who had less than two years’ experience and for some it was their first fire survival guidance call. The incident should, therefore, have prompted careful consideration about how best to manage multiple fire survival guidance calls.
Regrettably, we have come to the conclusion that despite all the indications that a large number of calls seeking fire survival guidance could be generated by a single incident, particularly one involving a large or high-rise residential building, the LFB failed to recognise that possibility and therefore failed to take any steps to prepare for it by training its staff or putting in place systems and procedures to respond to such an eventuality. The result was that when faced with an unprecedented number of callers from Grenfell Tower seeking fire survival guidance, the control room and those at the fireground were unable to rely on tried and tested systems and were forced to resort to various improvised methods of varying reliability to handle the large amount of information generated. That represents a major failing on the part of the LFB.
Taking emergency calls from the public, particularly those who are directly affected by a fire or other life-threatening event, and passing essential information quickly and accurately to those who need to receive it requires reserves of character and effective training. Control room staff receive training when they are recruited, but they also need regular training to ensure that their skills are kept up to date and that they benefit from any advances in learning. In the Phase 1 report the chairman was critical of some of the ways in which CROs handled emergency calls. He also identified various deficiencies in the Reference Information Files (RIFs) provided for the assistance of control room staff.[1041] We have therefore examined the way in which the LFB managed the training of control room staff in the years preceding the Grenfell Tower fire.
Ultimate responsibility for control room training lay with the senior officers, primarily AC George and AC Brown,[1042] but none of them exercised very much oversight of it.[1043] AC Brown delegated to POM Hayward responsibility for monitoring control room training and ensuring that the training needs of control room staff had been properly identified and effectively met.[1044] POM Hayward in turn delegated that responsibility to the SOM in charge of the Operational Support Team,[1045] who was responsible for identifying the training required, deciding its content and ensuring that it was delivered effectively.[1046] The SOM took full responsibility for training and did not need to obtain the approval of POM Hayward for training packages that were developed.[1047] The Operational Support Team was responsible for creating, organising and delivering all training documents and training packages for new entrants to the control room and existing staff.[1048] In the period between 2009 and 2019 the SOMs responsible for training were Lindsay Turner (2009–2012), Victor Bagnelle (2012–2015) and Joanne Smith (2015–2019).[1049]
POM Hayward generally adopted a laissez-faire style of management under which he did not expect to receive reports on matters relating to training unless there was a problem.[1050] He therefore did not actively monitor training; he expected the SOM to tell him if there was a problem of some kind.[1051] Otherwise, he assumed that the Operational Support Team was carrying out its job properly.[1052] In practice, POM Hayward’s monitoring of training was confined to discussions with the SOM about problems as they arose and the observation of some training.[1053] He did not regularly inspect the training records, despite the provisions of PN164, which contemplated that he would do so.[1054] He made none of the decisions about the content of control room training, nor did he consult AC Brown, AC Chandler or AC George about it.[1055] He expected any problem with training to be raised at Brigade Control Management meetings or in his meetings with the SOMs,[1056] but apparently none ever had been.[1057] In the absence of any problems he felt confident that the SOMs were managing training properly.[1058] For their part, neither AC Brown nor AC Chandler nor (to a lesser extent) AC George, exercised any active supervision of his oversight of training or monitored what he was doing to keep abreast of it.
In our view, such a detached approach to training should never have been allowed. Although POM Hayward was entitled to delegate the delivery of training to senior managers whom he knew and trusted, he had a personal responsibility to satisfy himself that the training programmes were suitable and were being delivered appropriately. He also had a personal responsibility to satisfy himself that the training was effective. As far as we can see, he did none of those things.
Most of the training was delivered to staff on watch. Accordingly, if during training there was a significant incident or a significant increase in the number of calls, staff could be recalled to their positions in the control room.[1059] Generally, training took place in a side room of the premises at Merton where the control room was located.[1060] When training had been completed, it should have been recorded manually by the Operational Support Team in a spreadsheet. From April 2019 it was recorded electronically in a system called System Training Evaluation and Performance (STEP).[1061]
The Lakanal House Board was responsible for the introduction of a programme of fire survival guidance training introduced in response to the Lakanal House fire.[1062] The relevant pre-inquest actions were action 8 (involvement of fire safety officers in training), action 11 (ensure that initial training on handling fire survival guidance calls complied with national guidance) and action 12 (provide refresher training on handling fire survival guidance calls).[1063]
National guidance on fire survival guidance training for CROs was published by the Home Office in 1993 and 1994 respectively in the form of FSC 10-93 and ‘Keeping People Safe’,[1064] to which we have referred. FSC 10-93 provided that recruits with between 8 and 12 weeks of service should be given fire survival guidance training to enable them, when dealing with callers trapped in domestic accommodation, to make a proper assessment of the situation, give appropriate advice where necessary and otherwise assist in minimising the danger to the caller.[1065] FSC 10-93 also recommended that continuation training be provided to CROs, which should include the fire survival guidance training set out in Appendix B.[1066] Appendix B recommended that fire survival guidance training should be presented by a fire safety officer and a fire control officer jointly and should comprise a lecture lasting one to one-and-a-half hours followed by a practical role-play session.[1067]
One of the key recommendations of ‘Keeping People Safe’ was that fire survival guidance refresher training should be undertaken at intervals of no more than 12 months.[1068] The training emphasised the need for an assessed role-play session in which CROs should actively participate.[1069] Its purpose was to test the ability of CROs to establish whether a caller can leave the building, recognise unusual responses, determine the caller’s location and provide appropriate guidance by following a sequence of prompts.[1070]
After the Lakanal House fire, the LFB created an initial fire survival guidance training package in 2010 for all control room staff which consisted of three training presentations[1071] entitled Building Types and Concepts,[1072] Fire Survival Guidance[1073] and Fire Survival Training: Introduction to Fire and Human Behaviour.[1074] SOM Lindsay Turner was responsible for drafting the new training package, although the senior management team as a whole was involved in decisions about it.[1075]
In 2010, fire survival guidance training was delivered to all control room staff, except those on long-term absence.[1076] A full day was allocated for it, off the watch. It was delivered by one of the trainers and included opportunities to ask questions.[1077] Half of the training was delivered by the Fire Safety team, in accordance with national guidance.[1078] At a meeting on 15 September 2010, the Lakanal House Board was informed that all control room staff had received refresher fire survival guidance training which had been fully in accordance with FSC 10-93.[1079]
In February 2010, before the fire survival guidance training package had been provided to staff, POM Hayward asked for role-play to be introduced as part of an assessment at the end of the week to consolidate the training and to give CROs an opportunity to practise giving fire survival guidance in a controlled environment.[1080] As a result, the fire survival guidance training in 2010 included active role-play, in which the trainer would act as the caller and a CRO would take the call.[1081] The trainer would improvise a situation based on their own experience and act out a fire survival guidance call to which the CRO would be expected to respond.[1082] No specific responses were required but the trainer was expected to ensure that the trainee followed the structure set out in the fire survival guidance RIF.[1083]
The initial fire survival guidance training package was outdated, being based on a fatal fire in the West Midlands in 1990 which had prompted the dissemination of FSC 10-93 and the ‘Keeping People Safe’ training. It was flawed in a number of respects. First, none of the initial training presentations referred to the Lakanal House fire or to the rapid spread of fire that had occurred on that occasion and the dangers involved.[1084] SOM Smith could not explain why that was the case[1085] and the 2011 training did not remedy the omission.[1086]
Secondly, none of the training presentations enabled CROs to understand significant features of modern buildings, such as cladding systems, and how they could contribute to a rapid and unusual spread of fire.[1087] It was a serious oversight not to have referred to the Lakanal House fire and modern methods of construction to ensure that control staff understood the relevance and importance of the training.
Thirdly, neither the 2010 nor the 2011 presentations complied fully with national guidance. FSC 10-93 warned that, in situations where the caller was prevented from escaping, CROs needed to be aware that reassuring the caller might not be appropriate and in some circumstances might even be dangerous.[1088] Yet the 2010 training presentation told CROs to reassure the caller, to remain positive in order to create a bond and to provide reassurance by saying that the firefighters were on their way and would be there very soon.[1089] SOM Smith was “extremely surprised” that the fire survival guidance training provided to CROs in 2010 included that advice and accepted that it reinforced bad practice.[1090] The advice to create a bond with the caller was removed from the 2011 training package, but that version still encouraged CROs to reassure the caller by telling them that the firefighters were at the scene.[1091] POM Hayward accepted that that was contrary to national guidance but could not explain why it had been included.[1092]
Fourthly, neither the 2010 nor the 2011 training presentations addressed some of the problems that CROs had encountered in connection with the Lakanal House fire, such as difficulty in identifying a safe room or problems in understanding the layout of the flat caused by the caller’s moving between rooms or even between flats.[1093]
Fifthly, neither the 2010 nor the 2011 presentations referred to FSC 54-04 or the need to ask specifically about the caller’s age, gender, ethnicity or mental or physical ability.[1094]
In August 2011, POM Hayward asked SOM Smith to review the fire survival guidance training packages to ensure that they were consistent with FSC 10-93.[1095] SOM Smith did not review the role-play exercise,[1096] but she did review the 2011 version of the fire survival guidance training presentation and concluded that it was materially incomplete, in particular, because it used neither the definition of a fire survival guidance call found in PN539 nor that found in current national guidance.[1097] However, her criticisms, which were bluntly expressed, were not acted on. SOM Smith could not explain why, in August 2011, more than two years after the Lakanal House fire, fire survival guidance training for CROs still contained the errors she had identified.[1098]
A new fire survival guidance training presentation was created in 2012, but most of SOM Smith’s comments were not acted on and the contents of the presentation were substantially similar to those of the 2011 version.[1099] SOM Smith could not explain why that was the case.[1100] She thought she had discussed her criticisms with POM Hayward but there is no record of any such discussions having taken place.[1101]
The history of this matter only reinforces our view that POM Hayward failed to exercise proper control over the development and delivery of training. The fault does not lie solely with him, however, since more senior officers should have been taking responsibility for ensuring that a matter of such importance was being properly managed.
On 3 August 2010, SM Stephen ‘Ned’ Kelly completed an audit of the Training team’s systems for managing the quality of training courses and assessing the performance of trainees, using the fire survival guidance refresher training course as an example.[1102] Having witnessed some practical role-play exercises, he noted that each candidate was exposed to a single fairly simple fire survival guidance call lasting between 90 seconds and two minutes, during which their performance was monitored.[1103] He made a number of criticisms, noting in particular that each trainee took part in only one fairly straightforward exercise and that the assessment of their individual performances was very informal, there being no documented note of what was expected of them or any record kept of their performance. He therefore recommended that the role-play element of the training be reviewed and that a robust assessment process be implemented.[1104]
POM Hayward told us that the control room had implemented some, though not all, of SM Kelly’s suggestions to improve the assessment of trainees’ performance.[1105] Four fire survival guidance role-play exercises were produced in 2011, for which a document was provided to enable CROs’ performance to be recorded and assessed.[1106] However, the control room did not implement any of his other recommendations because they considered that the course was already long enough.[1107]
The Lakanal Control report noted that at the time of the Lakanal House fire there had been a lack of structured, regular fire survival guidance training.[1108] The Lakanal House Board decided, therefore, by way of pre-inquest action 12, that a recurring programme of fire survival guidance refresher training should be established for all control personnel in accordance with national guidance.[1109] At a meeting of the Board on 15 September 2010, Commissioner Dobson noted that one of the areas that needed to be considered was to ensure that refresher training for the control room on handling fire survival guidance calls was maintained and recorded on STEP.[1110] Despite his comment, however, nothing appears to have been done, either to maintain refresher training or to record it on STEP.
National guidance required that refresher training on fire survival guidance calls should take place at least every 12 months and should include the training described in Appendix B of FSC 10-93. It recommended that training be delivered jointly with a fire safety officer and include active practical role-play.[1111] FSC 10-93 also recommended that refresher training be given systematically on the watch to all CROs, and should be scheduled and monitored.[1112] It emphasised that such training should cover little-used procedures and areas of weakness.[1113] AC Brown and SOM Smith accepted that fire survival guidance was a little-used procedure and SOM Smith accepted that the LFB’s response to the Lakanal House fire had demonstrated that it was an area of weakness.[1114] For those reasons AC Brown accepted that the need for fire survival guidance refresher training should have been made clear to CROs.[1115]
The programme of fire survival guidance refresher training was approved at the Lakanal House Board. In the second half of 2010, it was decided that there should be a two-year refresher training programme, under which a full day of classroom training would be delivered in the first year and a computer-based training package in the second.[1116] It was always intended that the full day of refresher training would include active role-play and would be delivered jointly with the fire safety team.[1117] The plan was that in alternate years CROs would complete the computer-based training package on their own,[1118] the intention being for them to be allocated time to complete it while on the watch.[1119] There was no plan to provide role-play exercises in the years when the computer-based training package was delivered; instead, CROs would be asked to complete a questionnaire designed to test their understanding of the principles involved.[1120] The intention was to deliver the first computer-based training package in 2011.[1121]
The two-year programme did not comply with national guidance because it did not provide for annual fire survival guidance training delivered jointly by a fire control officer and a fire safety officer and did not include an annual role-play exercise. Although the Lakanal House Board formally approved it,[1122] there was no discussion at its meetings about whether the programme complied with national guidance.[1123] At the meeting of the Lakanal House Board on 8 November 2010 action 12 was marked as “complete” because a system for delivering training had been established.[1124] The Board did not continue to exercise oversight of the action despite the continuing nature of refresher training.
AC Brown thought that the biennial programme was a reasonable and efficient approach to training.[1125] He regarded delivering a full day of classroom training every year as a significant workload for a team that was already delivering other training.[1126] SOM Smith, on the other hand, did not think that a two-year training programme was appropriate and expressed her concerns to Scott Hayward and Lindsay Turner.[1127] POM Hayward said that a two-year programme had been adopted to allow other training to take place.[1128] SOM Smith also pointed to the need for CROs to continue working while training was being provided.[1129]
Although we understand the difficulty of making CROs available for training, we do not think that it was sufficient to justify a two-year programme, given the weaknesses in providing fire survival guidance exposed by the Lakanal House fire and the fact that SM Kelly’s audit had revealed the need to strengthen the role-play element of training. The training required would take one day and SOM Smith accepted that it was possible to arrange shift patterns in a way that would allow training when staff were off duty, as had been done with training for the Vision system.[1130] In the circumstances, we do not think that POM Hayward was right to conclude that a one-day training course each year would exclude other important training.
Finally, in the Lakanal Control report the LFB told the coroner that a two-year refresher training plan, which had an active role-play element to it, had been put in place.[1131] However, by the time of the inquests in January 2013, it is clear that training of the kind that had been described was not in fact being provided. The LFB failed to notify the coroner that, in this respect at least, its intentions had not been realised, and no satisfactory explanation was given for that failure.
In the event, refresher training on fire survival guidance was not delivered as intended. In 2011 the computer-based training package that it had been intended to deliver to CROs that year was still under development and was therefore unavailable.[1132] As a result, POM Hayward approved the use by staff of the materials they had used in their initial fire survival guidance training.[1133], [1134] The course was not led by trainers but was designed for CROs to study alone for about an hour to an hour and a half.[1135] It is likely that staff undertook the training on the watch during the four-hour rest period that became available after the shift patterns had changed.[1136] The training plan for 2011 did not include active role-play, but CROs used call scripts and the RIF[1137] to confirm their understanding of procedures.[1138] However, the exercise did not involve active role-play and the performances of the CROs were not assessed.[1139]
POM Hayward provided us with information about the number of CROs who had undergone fire survival guidance training between 2011 and 2017.[1140] He accepted that the figures might not be entirely accurate and AC George and AC Brown both cast doubt on their reliability. However, we think they provide a helpful indication of the numbers who had received fire survival guidance training during that time. The evidence indicates that 94% of the available control room staff received training in 2011,[1141] but when compared to later years the figure looks very high. POM Hayward could not explain it and we have some doubt about its accuracy.[1142]
In 2012 CROs should have received a full day of fire survival guidance refresher training, including active role-play.[1143] However, in that year the provision of training was much reduced. The role-play element of the fire survival guidance refresher training was changed to a passive exercise in which staff were required to listen to pre-recorded simulated fire survival guidance calls and discuss their positive and negative aspects.[1144] Either SOM Turner or SOM Bagnelle (it is not clear which) approved the change,[1145] which was made in response to indications from staff that they felt very uncomfortable taking part in that element of the training.[1146] POM Hayward told us that he had not been consulted about the change and had not been aware that it had happened. He did not think that embarrassment was a sufficient reason for abandoning role-play, which he thought was an effective way of confirming CROs’ understanding of the training.[1147] This episode only goes to reinforce our criticisms of POM Hayward’s management of the control room.
At about the same time, the length of fire survival guidance refresher training was reduced.[1148] Instead of a whole day off the watch, the training took place during a four-hour short shift.[1149] The decision to reduce the length of the training was made by SOM Bagnelle without reference to POM Hayward.[1150] POM Hayward said that the same training had been delivered but that by reducing the number of breaks and the number of staff involved, it could be condensed into a four-hour period.[1151] However, that ignores the fact that the content was much reduced because there was only a brief discussion about difficult calls, as opposed to the one and half hour discussion originally included, and the element of active role-play was removed.[1152] Passive role-play reduced the time it took to complete that part of the training because a group discussion was substituted for individual participation.[1153]
In addition, fire safety officers were withdrawn from delivering the training. From 2012 onwards, fire survival guidance training for control room staff was intermittent and did not comply with national guidance. As a result, the refresher training that had been approved by the Lakanal House Board was not implemented.
POM Hayward said that he had become aware of the change to the training only during the Lakanal House inquests,[1154] but the evidence suggests that AOM Sharp had told the control room senior management team, including POM Hayward, about the change to the fire survival guidance role-play in September 2012.[1155] POM Hayward did not recall either having received her message or having discussed the proposal with AOM Sharp.[1156]
When on 5 February 2013 POM Hayward discovered that the duration and content of the fire survival guidance training had been changed, he asked SOM Bagnelle, who was by then the SOM in charge of training, how it had come about.[1157] AOM Sharp and SOM Bagnelle told him that the reason for the change was to prevent staff from being taken off duty[1158] and because there were not enough staff on duty between 08.00 and 14.00 to allow training to take place before the afternoon.[1159] POM Hayward said that nobody had told him that staffing difficulties prevented training taking place for a whole day.[1160] He had been aware generally that there were staff shortages and had understood that there were often no staff available to carry out training,[1161] but said he had never thought that training might need to be cut back as a result.
On or about 7 February 2013, during the course of the Lakanal House inquests, POM Hayward spoke to AC Brown about the changes to fire survival guidance training.[1162] AC Brown told him that he was very unhappy about the changes, particularly as the Lakanal Control report had said that the LFB was carrying out a full day’s training with active role-play.[1163] Although AC Brown intended to provide the coroner with information about the changes to fire survival guidance training,[1164] it is unclear what, if anything, was done.
AC Brown expected the biennial plan for fire survival guidance training to be reinstated with a full day of training every other year and a half day of computer-based training in alternate years.[1165] On the instructions of AC Brown, POM Hayward directed SOM Bagnelle to ensure that the active role-play was reinstated in accordance with SM Kelly’s recommendation in August 2010.[1166] However, POM Hayward did not instruct SOM Bagnelle to change the duration of training from four hours to a full day as AC Brown had expected.[1167]
Despite AC Brown’s instruction, active role-play was not reinstated.[1168] The episode illustrates our broader concerns about the LFB’s management systems at the time. POM Hayward should have been made aware of the change to the role-play exercise.[1169] Equally, once he had become aware of that change, it should have caused him to question the effectiveness of his supervision and monitoring of training.[1170] Had he done so, the failure to reinstate an element of active role-play in fire survival guidance training might have been identified and cured in time to make a significant difference to the performance of the control room in response to the Grenfell Tower fire.
In early 2012, AC Brown and AC Turek decided that fire safety officers did not need to deliver fire survival guidance refresher training.[1171] The decision was inconsistent with both national guidance (FSC 10-93) and pre-inquest action 8.[1172] AC Brown explained that the decision coincided with a restructuring of the brigade (including the Fire Safety department)[1173] and reflected the view that using fire safety officers to provide training on fire survival guidance was an unnecessary use of resources. There was a dedicated control room training team to provide that training and fire safety officers could be better employed inspecting premises.[1174]
AC Brown and AC Turek were satisfied that the fire safety officers had had sufficient involvement in the design and content of the new fire survival guidance training and they continued to be involved in the training of new control room staff.[1175] AC Brown also appears to have thought that as fire safety officers had been involved in a full day of fire survival guidance training in 2010, that was sufficient.[1176] However, national guidance required the contribution of a fire safety officer to each refresher training session and the longer CROs remained in their roles, the greater the importance of refresher training. At all events, the training team subsequently provided training without any contribution from a fire safety officer.[1177] AC Brown may have had confidence in the competence of the trainers, as he said he did, but we find it difficult to identify any steps that he had taken to satisfy himself of their ability to teach matters relating to fire safety.[1178] Although AC Brown said that he had relied on his personal knowledge of the members of the team and information obtained from senior managers, POM Hayward did not remember ever having discussed the withdrawal of fire safety officers with him.[1179]
Between 2013 and the Grenfell Tower fire, existing control room staff did not receive the full day of fire survival guidance refresher training that had been planned and approved by the Lakanal House Board and promised to the coroner.[1180] Some of the CROs were given training relevant to fire survival guidance, such as reviewing the RIF for Operators. They were also given some informal training and were involved in command unit training exercises, but none of that reflected the training that national guidance recommended.[1181]
The command unit training exercises involved units attending the control room at Merton and carrying out exercises to test activities such as two-way communication between the control room and the incident ground.[1182] The exercises had an element of role-play because CROs were required to take calls on the mobilising system and ensure that the information was passed to the command unit.[1183] However, the training was not designed for control room staff and those who took part did little more than help train the crews of the command units.[1184]
Some computer-based training was available, but not all CROs were able to take advantage of it due to technical problems that had not been resolved by the time of the Grenfell Tower fire.[1185] Moreover, the content of the fire survival guidance presentations used in the computer-based training was out of date, not having changed between 2013 and 2017.[1186] As POM Hayward accepted, the system for delivering them deteriorated as the presentations improved.[1187] The Operational Support Team did not create an alternative training opportunity for CROs who could not obtain access to computer-based training.[1188] SOM Smith’s preference was to introduce a computer-based training package because of the shortage of staff, particularly due to the introduction of Vision,[1189] but that made little sense in the face of the long-standing technical problems. Sessions led by trainers without the need for computer resources had been tried previously with only partial success. AC Brown said he had been taken by surprise to discover in 2016 that computer-based training had still not been implemented, but he refused to accept that the failure to implement the recommendation made in 2010 to introduce computer-based training for all control room staff on fire survival guidance reflected a chronic failure of management.[1190]
Assuming that the statistics produced by POM Hayward are broadly correct, the number of control room staff involved in fire survival guidance training, such as it was, between 2013 and 2017 was strikingly low. In 2013 and 2014, only 28% and 29% respectively of control room staff received any form of training.[1191] In 2015, no fire survival guidance training was carried out at all because of the introduction of Vision.[1192] In 2016, only 46% of control room staff received fire survival guidance training, and by the time of the Grenfell Tower fire in 2017, no fire survival guidance training at all had been delivered to any existing control room staff member that year.[1193]
POM Hayward explained that in 2013 the LFB’s priority had been to ensure that its new mobilising system, Vision, was working, as they had initially been given less than 14 months to deliver it.[1194] We shall return to Vision, but it is sufficient for present purposes to note that its introduction was a significant undertaking, which diverted attention from chronic problems affecting the management of fire survival guidance calls and related training. The control room also suffered from significant staffing problems and underwent restructuring between 2009 and 2017.[1195] During that period, none of the senior control room managers sought to take stock of training needs or take steps to ensure that all necessary training was given.[1196]
In January 2015, when SOM Smith returned from her secondment to the Chief Fire Officers Association, she assumed responsibility for the Operational Support Team and control room training.[1197] She asked for a list of CROs who had fire survival guidance training outstanding. She thought she must have received one, but had no specific recollection of it.[1198] We were not shown any such list.
On returning to her position in the control room SOM Smith had a handover discussion with SOM Bagnelle, but it did not touch on the numbers of control room staff who had received fire survival guidance training during her time on secondment (i.e., from September 2012 to January 2015).[1199] She was not told that the number of staff receiving fire survival guidance training had collapsed in 2013 and 2014,[1200] nor was she told about the changes that had been made to the training or that active role-play had been changed to passive role-play in 2012.[1201] She was unaware that in 2013 and 2014 fire survival guidance training had been limited to CROs reviewing presentations and being involved in command unit training sessions.[1202] She was told that fire survival guidance training had been reduced from a full day to four hours,[1203] but she did not ask why training had not been delivered as originally planned. She assumed that appropriate training had been provided while she had been away.[1204]
In 2015, SOM Smith discovered that there were not enough trainers to provide fire survival guidance training in the way that had been intended in 2011.[1205] Although she asked POM Hayward to make additional resources available to the Operational Support Team and two or three members of staff were seconded from the watch, they were required for training on Vision and were not available for fire survival guidance training.[1206]
From the latter part of 2016, SOM Smith monitored fire survival guidance training because she was trying to revise the computer-based training packages and resolve the problems with access.[1207] It is not clear why she had not been doing that from the time she returned in January 2015. During 2017, she worked with the training team to create a new fire survival guidance refresher training package which was due to be delivered in September 2017,[1208] but it did not lead to an increase in the number of CROs being trained in fire survival guidance or to any improvement in the content of the training.
Although the LFB could not reasonably have foreseen the considerable difficulties that were encountered in implementing Vision, that does not excuse the failure of the senior officers responsible for the operation of the control room, namely, SOM Smith, POM Hayward and AC Brown, to keep fire survival guidance training under close review and, in particular, to decide how to deliver such training once it became clear that the problems flowing from the introduction of Vision were dominating the control room’s attention, time and resources.
Despite the failure to deliver fire survival guidance refresher training, neither POM Hayward nor AC Brown informed the Lakanal House Board, the Lakanal House Working Group or the co-ordination board that training had fallen far short of that which had been approved and promised to the coroner.[1209] It seems that no one in senior management was aware of the true scale of the failure to provide fire survival guidance training between 2012 and 2017. For example, in January 2013, AC Brown told AC Dexter that 94 out of 104 staff had been given fire survival guidance refresher training.[1210] That figure, which amounted to 90.4% of staff, was far in excess of the figure of 61% provided by POM Hayward in his witness statement,[1211] but although the basis of his figure of 90.4% could not be identified, AC Brown remained confident that training had been taking place. He thought that any apparent shortfall in numbers was attributable to poor record-keeping.[1212]
In his review of the Lakanal pre-inquest actions in June 2013, AC Chandler said that the refresher training programme had been put in place and that no further action was required.[1213] The Chandler review was sent to AC Brown and POM Hayward for information,[1214] but POM Hayward did not correct him and provide the true picture.[1215]
In 2014, Adrian Bevan, an LFB health and safety manager,[1216] asked for information from AC Brown about control room training to enable him to answer a request from the Health and Safety Executive for information on control room practices, procedures and training following the Lakanal House inquests.[1217] On 3 July 2014, AC Brown told Mr Bevan that between February 2011 and June 2014 277 individual fire survival guidance training sessions had been delivered by senior control room officers in addition to the regular watch training sessions.[1218] However, although the source of that particular statistic is not clear,[1219] it is plain that POM Hayward did not tell AC Brown that by July 2014 fire survival guidance refresher training was being given to less than a quarter of control room staff.[1220] It is also notable that the Health and Safety Executive was not told that since 2012 fire survival guidance training had not met national guidance in some material respects.[1221]
AC Brown accepted that he did not know how many CROs were actually being trained in fire survival guidance at the time, but he said that after his discussions with POM Hayward and the CROs he had been left with the impression that fire survival guidance refresher training was being delivered where practically possible.[1222] However, at no stage did POM Hayward ever provide AC Brown with a reliable record of fire survival guidance training, which would have enabled it to be effectively monitored, and AC Brown never asked for one.[1223] Nevertheless, AC Brown was aware of periods during which fire survival guidance refresher training was not being provided as had been agreed – for example, between 2015 and 2017, when the training of control room staff concentrated on the Vision mobilising system.[1224] Although he accepted in the light of the Lakanal House fire and the findings of the Mayor’s Office for Policing and Crime[1225] (to which we refer later) that fire survival guidance training was of critical importance, AC Brown sought to justify its absence on the grounds that all available resources had been taken up by the need to train staff on Vision. He maintained that the quality of the control room’s response to fire survival guidance calls had been kept under continuous review.[1226]
The introduction of Vision clearly made great demands on the resources available for training, but the fact remains that there was a chronic, systemic failure to ensure that effective fire survival guidance refresher training was consistently provided to all control room staff. Such quality assurance as existed had signally failed to identify the fact that, from 2012 onwards, the number of CROs receiving such training was low. There was a consistent failure to comply with national guidance or with the assurances given to the coroner.
In July 2016, at the instigation of AC Brown, AC George carried out a review of the control room, but did not identify fire survival guidance training as an area of concern.[1227] It had not been included in his terms of reference,[1228] which had been informed by discussions with staff between September and November 2015.[1229] In these discussions, CROs had not expressed concern about the lack of fire survival guidance training[1230] or about their readiness to handle fire survival guidance calls.[1231] AC George himself was not concerned about fire survival guidance training because when he started his review AOM Sharp had given him a schedule of planned training.[1232] He was not aware of the changes that had been made to the fire survival guidance refresher training by the Lakanal House Board;[1233] nor was he aware that in 2015 and 2016 training on Vision had, to say the least, placed severe restrictions on it.[1234]
AC George was confident that fire survival guidance training was taking place because he witnessed it in 2016 and early 2017[1235] and he was assured by AOM Sharp, POM Hayward and SOM Smith that it was being delivered.[1236] However, the training he witnessed was command unit training, which was not aimed at CROs, and he did not attend the training sessions himself, having simply seen from his office window a number of people and command units gathered outside.[1237] AC George did not examine the content of the fire survival guidance training packages and he had no direct knowledge of the extent to which they had been delivered in 2016 and 2017.[1238]
In the report of his review that he presented to the Corporate Management Board in February 2017 AC George said that additional familiarisation training on fire survival guidance had been given to all staff.[1239] Insofar as that gave the impression that additional fire survival guidance training had been provided to all CROs since his first report in July 2016,[1240] it was misleading. AC George accepted that, as head of the Operational Response department and, from March 2017, Director of Operations, he should have been aware of the consistent failure to provide fire survival guidance training to CROs in 2016 and 2017[1241] and that that failure was both chronic and systemic.[1242] He said that POM Hayward and SOM Smith had regularly told him about the problems being encountered with Vision, which had crowded out other training,[1243] but there is no evidence that he made any effective effort to ensure that regular and structured fire survival guidance training was provided.
The importance of fire survival guidance refresher training cannot be over-stated. The senior officers responsible for the control room plainly understood the need to give priority to such training, particularly because of the weaknesses in handling emergency calls exposed by the Lakanal House fire in 2009. At that time no structured or regular fire survival guidance refresher training was being conducted by the LFB and at the time of the Grenfell Tower fire in June 2017 that remained the case. The failure to provide CROs with regular fire survival guidance refresher training is undoubtedly a serious indictment of the LFB. Even allowing for the difficulties resulting from the introduction of Vision, there is no justification for such a longstanding failure to address a vital element of the control room’s work that was well known to senior management.
Even though the Lakanal House fire demonstrated the real danger to life posed by the failure to provide effective fire survival guidance training, the fact is that none of senior officers responsible for the operation of the control room ever tackled the challenge of providing the necessary training with the seriousness or dedication it deserved.
The need to monitor and manage the performance of CROs, particularly in relation to handling fire survival guidance calls, was identified in the Lakanal Control Report, which recommended the introduction of a policy identifying the standards that staff were expected to reach and how performance would be assessed and monitored, particularly in relation to calls where fire survival guidance was given.[1244] That recommendation was said to have been implemented by senior managers’ undertaking a review of all high-rise or fire survival guidance calls and amending the RIFs and training packages to ensure that they reflected FSC10-93 and ‘Keeping People Safe’.[1245] Although it did not give the impression that a new policy of the kind envisaged by the recommendation had been introduced, the statement was misleading insofar as it gave the impression that the omissions and flaws that we identified earlier had been put right.[1246] AC Brown explained the failure to introduce a policy of the kind contemplated by the recommendation by the fact that those with responsibility for the control room had revised the existing materials in a way that met the substance of the recommendation.[1247]
In late 2009, after the Lakanal House fire, a quality assurance system known as ‘Call Coach’ was introduced. At the suggestion of SOM Smith it was supplemented by a review of fire survival guidance calls to check whether the training introduced after the Lakanal House fire had been effective.[1248]
Call Coach was a structured system of reviewing and learning from the way in which CROs handled calls coming into the control room. In summary, a supervisor would choose at random from a short list of three calls at least one call a month for each call-handler and one call every three months for each team leader.[1249] The supervisor would listen to the call and assess the call-handler using a prescribed standard which included a scoring system.[1250] After the assessment, a meeting would be held between the call-handler (or team leader) and the supervisor to discuss and review the assessment.[1251] The supervisor assessing the call was then responsible for coaching the call-handler or team leader and monitoring the results obtained from successive assessments.[1252] SOM Smith was responsible for introducing the system,[1253] which had been operated monthly between 2010 and November 2015.[1254]
However, fire survival guidance calls were not included in the Call Coach assessments.[1255] The decision to exclude them appears to have flowed from an agreement between DAC Payton, then Deputy Assistant Commissioner for Control and Mobilising, and the trade unions.[1256] The reason for any such agreement is unclear, but it meant that supervisors did not have an opportunity to assess the quality of the response to fire survival guidance calls except when they supported a CRO handling such a call or during the fire survival guidance review process described below.[1257] Since assessment was not the purpose of the supervisor’s involvement, supporting a CRO during a fire survival guidance call did not amount to an effective form of monitoring and managing performance.
Call Coach provided supervisors with a degree of reassurance about CROs’ ability to handle calls, but POM Hayward did not think it was a particularly good system.[1258] However, partly because of the money that had been spent acquiring it and partly because of the time spent bringing it into operation, POM Hayward was not inclined to look into other ways of assessing those skills.[1259] SOM Smith was not aware of Operational Support Team’s analysis of the CROs’ performance and AC Brown did not ask her to consider the outcome of reviews.[1260]
In November 2015, when Vision was introduced, Call Coach became obsolete and was replaced by a new system called Neptune Intelligence Computer Engineering (Neptune).[1261] However, Neptune was not used to review call-handling by CROs and no formal arrangements were made to make up for the loss of Call Coach.[1262] No quality assurance review process was therefore in place to monitor CROs’ call-handling in the years leading up to the Grenfell Tower fire.[1263]
Following an incident, however, it was standard practice for senior managers on duty to review fire survival guidance calls.[1264] There was no policy or guidance document available to direct their reviews so they relied on their own experience and training.[1265] A description of the circumstances in which each call had been made and a summary of its contents were recorded in an electronic database, but the database did not include any comments critical of the call-handler.[1266] Although SOM Smith said that the database was of some value, for example, in identifying causes of concern or examples of good practice, the process did not amount to a systematic appraisal of the performance of CROs.[1267] There was no evidence of how the review was used or how it contributed to their training or development.[1268]
In addition to the review carried out by senior managers, SOM Smith reviewed every fire survival guidance call and every call from a high-rise building on the system[1269] to check that the correct advice had been given in accordance with FSC 10-93, and later, PN539.[1270] If deficiencies were found, the CRO’s line manager would take the necessary action.[1271] POM Hayward said that he and SOM Adam Crinion had also listened to the calls.[1272] However, the findings of SOM Smith’s review were not recorded anywhere and we have seen only a few of the reports that were provided to OMs and CROs about the handling of fire survival guidance calls.[1273] Those that we have seen are all positive and do not identify any mistakes in the way that calls were handled.[1274]
Although SOM Smith told us that the obligation to review fire survival guidance calls fell to the person on duty at the time a call was received,[1275] SOM Keith Diamond and SOM Bagnelle assumed that task after she had been seconded to the Chief Fire Officers Association in September 2012.[1276]
When SOM Smith returned to the LFB in January 2015, she did not ask SOM Diamond or SOM Bagnelle for a report on the fire survival guidance reviews they had undertaken in her absence,[1277] but she did resume her review of all fire survival guidance calls, relying on her expertise rather than PN539.[1278] By that time she found it had become impossible to review all the calls from high-rise buildings because the number of calls typically received by the LFB during high-rise incidents had become too great and her workload had increased with the introduction of Vision.[1279] She did not delegate the task to anyone else and was confident that the Operational Support Team had not had the capacity to take it on because its workload had also increased as a result of the introduction of Vision.[1280] Given that Call Coach had become obsolete at the same time, there was no review of CROs’ call-handling after 2015, apart from the limited and uncritical review described above. SOM Smith told us that a structured debriefing process had been in place since 2011 to enable CROs, supervisors and OMs to share and discuss their experiences following an incident.[1281] On any view, however, that was not the kind of independent review of call-handling that she had previously undertaken.
The absence of any effective arrangements for undertaking a critical review of the quality of responses to fire survival guidance calls compounded the pre-existing problem surrounding the correct description of a fire survival guidance call that the LFB had failed to resolve effectively. After Call Coach became obsolete in 2015, the LFB failed to introduce an alternative system for critically reviewing fire survival guidance calls to make sure that CROs were meeting the standard required by PN539. No good explanation was provided for that failure, which provides another example of the LFB’s continuing inability to recognise the importance of fire survival guidance calls in ensuring the safety of people affected by fire and smoke.
On 23 February 2012, the LFB issued a new policy, Policy No. 790 (PN790) ‘Fire survival guidance calls’ to replace PN155.[1282] It was an operational policy designed for use by firefighters and covered the exchange of fire survival guidance information between the control room and the incident ground.[1283] It was not designed for use by the control room itself, even though it had a significant bearing on the handling of fire survival guidance calls.[1284] It was developed primarily by SM Patrick Utting, working closely with SOM Smith throughout the drafting, consultation and approvals process.[1285]
Although PN790 recognised that a large number of fire survival guidance calls could be received during a single incident,[1286] it offered no guidance to control room staff on how best to respond to such a situation.[1287] Neither AC Brown nor any other senior officer asked POM Hayward to assess the effect of the new policy on the control room or to determine what training might be required as a result. AC Brown sought to justify that omission on the basis that the control room was used to handling many different incidents at the same time and that although fire survival guidance calls were different and not received very often, CROs used the same knowledge, skills and experience as they used on a daily basis when handling them.[1288] We cannot accept that. The seriousness of fire survival guidance calls and the fact that incidents giving rise to multiple fire survival guidance calls occurred relatively infrequently make it difficult to see how he could reasonably have considered them to be a part of normal business. The various failures in handling fire survival guidance calls identified by the LFB itself following the Lakanal House fire required a more considered approach to making sure that CROs were given as much help as possible in responding to the challenges presented by the need to handle several fire survival guidance calls at the same time. We do not understand why that never occurred to AC Brown or any other senior officer responsible for the control room.
Following its introduction, supervisors discussed PN790 with CROs to ensure that they were generally familiar with its contents, but no formal or structured training was provided.[1289] The training records indicate that only some of the control room supervisors themselves received any training on it.[1290] Although that may reflect poor record-keeping, that fact alone meant that the LFB had no accurate note of who had received training on the new policy and who had not.[1291]
Paragraph 8.7 of PN790 recognised that in exceptional circumstances an incident commander might consider informing control that the “stay put” advice to callers should be changed and that they should try to leave their property. At the same time, it warned the incident commander that such advice might be contrary to national policy for control staff engaged on fire survival guidance calls and that it would be necessary to communicate with the officer in charge at the control room to get agreement for such a change.[1292]
In the context of the Grenfell Tower fire that was an important provision. SOM Smith was the principal author of paragraph 8.7, so after the Lakanal House fire she was aware that “stay put” advice might have to be changed.[1293] However, even though she and POM Hayward were aware of that paragraph, they gave no consideration to training CROs on how to explain to a caller that the advice previously given had been changed.[1294] SOM Smith’s explanation for that failure was that the LFB did not think that in practice it would be necessary to do that.[1295] POM Hayward’s evidence echoed that of SOM Smith. He said that the LFB had not expected “stay put” advice ever to be withdrawn, so no training had been given on how best to respond to that situation.[1296]
It is impossible to reconcile the attitude displayed by POM Hayward and SOM Smith with the clear terms of paragraph 8.7. In effect, they simply ignored it and by doing so deprived those who worked in the control room, and thereby the LFB as a whole, of the training designed to prepare them for the challenges they would face if “stay put” advice had to be revoked. That was a very serious failure for which no plausible excuse has been offered. Moreover, the procedures that the control room would rely on if multiple fire survival guidance calls were received were never properly tested in a training exercise. After the Lakanal House fire a few training exercises were held to test the handling of fire survival guidance calls, and in particular, the arrangements for passing information to the incident ground, but none of them tested the effectiveness of the control room’s own procedures.
The first of those tests was the Heygate Challenge, held on 16 June 2011, which was designed to test the proposed amendments to the high-rise firefighting policy (PN633) and the new fire survival guidance policy (then PN155).[1297] Four fire survival guidance calls were used in the exercise.[1298] POM Hayward explained that the exercise had been designed to test communications rather than to assess the capacity of the control room to deal with a significant number of fire survival guidance calls.[1299] In other words, the focus was not on the training of CROs. No-one representing the control room appears to have had any influence on the number of fire survival guidance calls used. As we have noted in chapter 78, neither POM Hayward nor SOM Smith could explain why the exercise had assumed the existence of only four fire survival guidance calls, given that five had been received at the Lakanal House fire.[1300]
Although the magnitude of the challenge presented by multiple fire survival guidance calls was identified in the exercise, the LFB never organised an exercise specifically to test the number of calls that the control room could effectively handle.[1301] In view of the difficulties experienced by CROs in handling the five calls generated by the Lakanal House fire, no good reason was given for that failure.
The second exercise, held on 20 December 2012, was Exercise Florian, which simulated a fire on the seventh floor of a 15-floor purpose-built block of maisonettes, generating three fire survival guidance calls involving four persons, three of whom were rescued and one of whom escaped without assistance.[1302] The aim of the exercise was to find out how well PN790 worked in practice and whether it contained any defects.[1303]
However, the exercise did not focus on all aspects of PN790. For example, it did not practise the revocation of “stay put” advice or consider the consequences that might flow from that.[1304] Nor did it use the same number of fire survival guidance calls as had been received during the Lakanal House fire, although AC Brown thought that the three calls that formed the basis of Exercise Florian had reflected the three calls received simultaneously at the Lakanal House fire.[1305] He said that no consideration had been given to including more than five fire survival guidance calls in order to test the arrangements in PN790 because there was an unspecified exercise going on in the background in the control room, which simulated other incidents. AC Brown believed that together they would have put the control room under the same pressures.[1306] Even if that were so, however, the exercise did not address the important function of rigorously testing the arrangements for handling multiple fire survival guidance calls.
Unfortunately, Exercise Florian did not test the control room’s ability to handle a growing number of fire survival guidance calls.[1307] As with the Heygate Challenge, its focus was on the response of operational crews rather than the control room’s ability to handle multiple fire survival guidance calls. The CROs’ function appears to have been to assist in the exercise and act as observers rather than undergo training.[1308] Given the failings in handling fire survival guidance calls later identified in the Lakanal Control Report, appropriate training for the CROs should have been included in the exercise. One of the suggestions made following that exercise was that someone should turn the documents created for the exercise into a regular training programme.[1309] POM Hayward said that regular training took the form of training with the command units, which ran from mid-2013 until 2015 and again from mid-2016,[1310] but again, that training was not designed for the benefit of CROs.[1311] It appears, therefore, that no training was introduced for CROs following Exercise Florian.
The third exercise was Exercise Penfold, which was held on 14 November 2013.[1312] It simulated a ten-pump high-rise fire with several seats of fire and persons trapped on various floors.[1313] The exercise involved four fire survival guidance calls, to which the CROs were expected to respond using the RIF for guidance.[1314] An AOM was available to assist the CROs.[1315] Again, it is unclear why the decision was taken to limit the exercise to four fire survival guidance calls, given that five had been received at Lakanal House, or why the LFB did not seek to test the limits of PN790 by using more than five calls.[1316] After the exercise, it was suggested that AOMs and the OM be more directly involved in an exercise of that kind in order to practise their roles within fire survival guidance procedures, such as communicating directly with the fire survival guidance command unit.[1317] POM Hayward could not say whether that suggestion had been pursued.[1318] Following Exercise Penfold, no further exercise or training on PN790 was organised for CROs. At most, they were asked to assist at and observe command unit training exercises which practised communicating fire survival guidance information from the control room to the incident ground. Such exercises were not designed to benefit them.
Pre-inquest action 17 in the Lakanal Control report recommended that an enhanced fire survival guidance training package be developed for control room supervisors to enable them to provide support to CROs handling fire survival guidance calls to ensure a standard commensurate with national guidance.[1319] In June 2011, the Operational Support Team produced a training package for supervisors in response to that recommendation, supported by a slide presentation.[1320] The presentation stated that the supervisors’ main function was to support CROs taking fire survival guidance calls and to make sure that the information they gathered was passed to the incident commander or the command unit.[1321] It suggested ways in which a supervisor could support a CRO taking a fire survival guidance call, including ways of gathering relevant information from the caller.[1322] It also suggested ways in which a supervisor could assist in passing information to the incident ground, for example, by appointing a supervisor to act as the sole contact between the control room and the incident ground.[1323] The presentation contemplated that multiple fire survival guidance calls might be received but did not include any advice about how a supervisor should collate the relevant information and transmit it to the incident ground.[1324] The presentation included a list of prompts for information that should be collected and passed immediately to the incident ground, but did not refer to the need to remind the CRO to obtain information about any vulnerabilities the caller or others with them might have.[1325] POM Hayward said that CROs normally asked for information of that kind but that in any event they expected callers to volunteer it without needing to be asked.[1326] The training did not include any reference to the Lakanal House fire, nor did it identify any lessons to be learnt from it.[1327] Notwithstanding SOM Smith’s evidence to the contrary, the training does not appear to have been revised after November 2012 to reflect the reasoning and conclusions of the Lakanal Control report, despite its relevance to any supervisor who might need to manage the control room during an incident of that kind.[1328]
In 2014, the Operational Support Team developed another short training exercise for control room supervisors lasting between 30 and 60 minutes.[1329] It partly remedied one of the defects in the previous training by reminding supervisors that CROs should ask whether the caller was disabled, used a wheelchair or whether they were ill and used oxygen,[1330] but it did not tell supervisors to remind CROs that such information should be passed to the incident ground.[1331]
It is not clear whether the training we have described was provided to all supervisors.[1332] It seems clear, however, that they were not trained how to manage the control room during a large incident that gave rise to multiple concurrent fire survival guidance calls.[1333] Nor were they trained in how to deal with a major incident.[1334] That was another serious failure for which no satisfactory explanation was given.
There were a number of other causes, mainly of an organisational nature, that contributed to the failure of the LFB to provide the training and guidance needed by control room staff. One clear and consistent theme that emerged from the evidence was the existence of a perception within the control room and the wider LFB that the control room was a separate entity distinct and different from the rest of the brigade.[1335] That was reflected in the opinion of AC Jonathan Smith when he was instructed by the then Commissioner in July 2019 to undertake a root and branch review of the brigade’s control function.[1336] He concluded that the control room needed to be more closely integrated into the brigade, rather than exist as a separate and distinct part of the organisation, as it had become over time. In his view there needed to be a fundamental reappraisal of the position of the control room to ensure that it was given an importance equal to that enjoyed by other sections of the brigade.[1337]
The reasons for the isolation of the control room are complex, but were essentially historical, geographical and technological.
Originally, there had been a number of area control rooms across London, each located within an operational fire station. At some point they were consolidated and became based centrally at LFB headquarters in Lambeth.[1338] Throughout both those periods, therefore, control room staff were able to meet their operational colleagues on a daily basis.[1339]
In April 2004, the control room moved from Lambeth to Greenwich View Place on the Isle of Dogs and in January 2012 it moved again to a purpose-built London Operations Centre in Merton, which is its current location.[1340] When the control room moved to Greenwich View Place, CROs became physically separated from other staff within the organisation.[1341]
Technology also played a part in the separation. Over the course of time systems were introduced in other parts of the organisation which could not be used by the control room or were not properly adapted to its needs. The most significant examples are the Staff Attendance Recording System (StARS) and the STEP system.[1342] STEP, which was linked to StARS, was designed to enable a senior officer to review the training undertaken by junior officers and plan for future training needs.[1343] Although the rest of the LFB used STEP to record training, the control room was unable to do so because StARS could not accommodate its shift patterns. It was therefore obliged to use a spreadsheet to record information about training which was then added to STEP manually.[1344] In contrast to the live tracking available to operational staff on STEP, the information on the control room’s spreadsheet was added at monthly or quarterly intervals.[1345] It is not clear to us why the adjustment to StARS required to accommodate the control room’s shift patterns was not made before it was introduced.
AC George said that when he had started working with the control room in 2016 it was like going back in time ten years. The systems were out of date.[1346] He concluded that the control room had not kept pace with the rest of the organisation because managers had not ensured that the LFB’s systems operated as effectively for it as they did for fire stations.[1347] POM Hayward said that changes to the programming of STEP and StARS had been needed to accommodate the control room’s shift patterns, but that things had moved slowly.[1348] He said that he had asked for changes to be made, but had been told that other requirements took priority.[1349]
There was also a marked difference between the control room and the operational departments in the way that training was organised and procured. As set out above, in April 2012, the LFB entered into a contract with Babcock for most of its training requirements,[1350] but that contract did not extend to the training of control room staff. Their training was provided by the Operational Support Team[1351] and, as POM Hayward confirmed, there were no arrangements for assessing the quality of the training it provided.[1352] When SM Kelly reviewed the Training team’s quality assurance systems in 2010 he found that there was no general plan for ensuring that training was of the appropriate quality, but he identified various systems which enabled the team to assess the quality of the training it had provided. Among them was Call Coach, described above, which he considered to be a very effective tool.[1353] However, although his audit was based on fire survival guidance training, SM Kelly was apparently not aware that fire survival guidance calls were not monitored using Call Coach or any other system.[1354] As a result, he appears not to have appreciated that fire survival guidance calls were not subject to any quality review or assurance process.
In June 2013, AC Chandler reviewed the progress made by the control room in carrying out the Lakanal pre-inquest actions. He concluded that the training syllabus needed to be entirely refreshed and recommended that a fundamental review of training should be undertaken in 2015 or 2016.[1355] However, no such review was undertaken[1356] because of the overriding focus on implementing Vision.[1357] Although AC George covered aspects of training in his review of the control room, it did not amount to the fundamental reappraisal which AC Chandler had called for.[1358]
In the report into his review of the control room AC George had recommended that responsibility for control room training should be transferred to Babcock.[1359] Although that was considered, AC George and Angela Hale, the LFB’s Training Commissioning manager,[1360] subsequently agreed that the nature of the training required by control staff was so specific that there was limited value in employing Babcock and that it should be retained by the LFB.[1361] It was also decided that the Operational Support Team should continue to deliver that training, apart from certain computer-based training packages.[1362] As a result, control room training was not subject to any regular audit by either the LFB’s training department or any other organisation.
The Operational Support Team was in practice the only body within the LFB responsible for the development and delivery of control room training and for ensuring that it was of an appropriate standard. However, its members were not recruited as specialist trainers; they were all staff who had previous experience as CROs.[1363] Until 2016 or 2017, when they received a “train the trainers” course from Babcock, its members did not receive any formal training on how to create and deliver training packages.[1364]
SOM Smith had not received any training or preparation before assuming responsibility for the training function of the Operational Support Team and had not asked for any.[1365] In particular, she received no training in quality assurance,[1366] which is a cause for concern, given the absence of any regular or formal process for assessing the quality of training.[1367]
The control room’s isolation was increased by the marginalisation of its senior managers in brigade meetings. POM Hayward attended monthly Departmental Management Board meetings, at which AC David Brown met the DACs to discuss current matters affecting the brigade.[1368] POM Hayward said that the meetings had been mainly concerned with operational matters, to the point at which he did not always understand the subject-matter and did not contribute greatly to discussions.[1369] That was unfortunate for a number of reasons: first, because POM Hayward clearly felt isolated and ill-equipped to participate, and secondly, because they were one of the points of contact with POM Hayward on which AC Brown relied to be informed about the running of the control room.[1370] If POM Hayward did not participate effectively in the meetings, there was a risk that AC Brown would not have sufficient information to enable him to exercise effective management oversight of the control room.
The mobilising system enables CROs to carry out their core role of despatching crews to fight fires. As mentioned earlier, in 2015, the LFB changed the mobilising system used by the control room from ProCAD to Vision,[1371] a system which had been developed and delivered by a commercial company, Capita. Since the effective despatch of crews is the primary function of the control room, at least in the initial stages of the response, it was vital that staff received adequate training on the new system before it entered service.[1372]
Vision had been due to enter service in 2014, but the complexity of the LFB’s requirements meant that Capita was unable to deliver the system on time.[1373] From early 2013 the Operational Support Team started to prepare for its introduction.[1374] Initial training on Vision for existing control room staff took place between 24 June 2013 and 14 January 2014 and following further delays, tailored training for CROs continued to be delivered until the system eventually entered service on 17 November 2015.[1375]
The introduction of Vision resulted in a reduction in response times, with the result that appliances reached their destinations about 10 seconds earlier than had been the case when the control room had been using ProCAD.[1376] That was no doubt an improvement in performance, but, as AC George told us, the introduction of Vision had been extremely difficult for the control room.[1377]
For a number of years after its introduction, Vision continued to be plagued by significant system failures. More than 500 faults were reported to Capita in the first six months.[1378] There were also six occasions during the first year when the system failed altogether for periods of between 40 minutes and three hours, requiring the use of contingency measures.[1379] AC George described instances when the mobilising system slowed to the point of stopping completely, causing the CROs to resort to a secondary mobilising system that he described as “basically pen and paper”.[1380] That was extremely stressful for staff, who had occasionally left the control room in tears.[1381] The scale of the difficulties was such that in the period from 2016 to 2017 the Operational Support Team spent about 60% of its time reporting problems with Vision, revising training packages to reflect changes to the system and training staff on ways to circumvent problems. During the first two years in which Vision was in use, ways were devised to circumvent about 100 problems.[1382] Put briefly, between 2013 and 2017, the introduction of Vision generated a very substantial amount of additional work for the control room and the Operational Support Team in particular.
It was accepted by LFB officers that the task of implementing Vision had been all-consuming and had completely swamped the control room.[1383] One of the most significant consequences was its effect on training, which manifested itself in a number of ways.
One immediate consequence of the introduction of Vision was that all the control room’s training capacity was directed towards training staff on the new system. When SOM Smith returned from the Chief Fire Officers Association she was asked to create a plan to train all 100 staff in the control room on Vision,[1384] which was regarded as a priority. That meant arranging 2,000 hours of training on Vision before it went into service.[1385] Inevitably, resources were directed to ensuring that the system was effective as soon as possible.[1386] Between 2015 and 2017, most, and sometimes all, of the Operational Support Team’s resources were devoted to that task, because it was essential that the brigade had an effective mobilising system.[1387] POM Hayward said that the control room had been unable to plan any training until Vision was fully operational and officers could see how it performed.[1388] That applied even to areas where annual training was expected, such as fire survival guidance refresher training.[1389]
In order to cope with the pressure of work expected to result from the introduction of Vision, from 2014 and throughout its implementation the number of AOMs in the Operational Support Team was increased from four to six.[1390] The increase was originally expected to be temporary, but throughout 2016 the amount of work produced made any reduction impossible and the increase was made permanent by AC George in 2016.[1391]
The training requirements imposed by Vision did not cease when the system entered service. Minutes of a Brigade Control Management meeting on 8 December 2015 (about three weeks later) refer to a list of problems that Capita had already been asked to resolve and referred to staff having to work around problems with the paging system.[1392] From that point on, the minutes of Brigade Control Management meetings and the Joint Committee for Control Staff record concerns about the performance and stability of Vision.[1393]
The problem was not simply one of confidence in the system, because faults needed to be corrected as they were identified. Accordingly, it was necessary to make changes to the system, which in turn made it necessary to train CROs urgently on the revised version. Frequent amendments were very disruptive. On many occasions staff returned from their rest days to find that a change had been made to the system that required them to undergo immediate further training.[1394] The burden of training was both substantial and, until at least 2017, constant.[1395] The inevitable consequence was that other areas of training, including training on fire survival guidance, were delayed or deferred indefinitely. POM Hayward said that no fire survival guidance training at all had been given in 2015 because of the introduction of Vision.[1396] In 2015, the control room had been concentrating entirely on implementing Vision and therefore no other training had been given.[1397]
POM Hayward told AC Brown that there were occasions when fire survival guidance refresher training had not been delivered in accordance with the agreed programme, for example, between 2015 and 2017 while the CROs were being trained on Vision.[1398] The explanation AC Brown gave us for allowing that situation to continue was that Vision was a critical project and that it had been essential to deliver it on time.[1399] He did not agree, however, that all other training had ceased as a result.[1400] AC George had also been aware of the general adverse effect that Vision was having on control room training, although he too said that he had not been specifically informed of its effect on fire survival guidance training.[1401]
Training on Vision also put a temporary halt to the command unit training on fire survival guidance in which the control room had been involved. POM Hayward said that that training, which had run since mid-2013, had been stopped in 2015 because of the demands of Vision, although it had been resumed to a limited extent in mid-2016.[1402] Staff training and development as a whole was adversely affected.[1403]
It is not clear what, if anything, was done to mitigate the effect on other areas of training of introducing Vision. AC George said that the sheer volume of work needed to implement Vision made it extremely difficult to devote resources to other training.[1404] It does not appear that consideration was given to evaluating the competing priorities of training on Vision and other forms of training, including training on fire survival guidance, until after Vision had become operational in 2015.[1405] POM Hayward said that at that point the control room had taken stock of the training needs of staff and had examined how they could run more general training as well as the continuing training on Vision.[1406]
The fundamental review of training proposed by AC Chandler in June 2013 did not take place because of the overriding concentration on getting Vision into service.[1407] Although AC George covered aspects of training in his review of the control room, it did not amount to the fundamental reappraisal for which AC Chandler had called.[1408]
It is clear that the introduction of Vision was a significant challenge for the LFB, particularly for the control room, and required a substantial amount of work to stabilise the system. Its success in reducing the average time taken for an appliance to arrive at an incident together with other operational benefits came at the cost of a reduction in the ability of the control room to provide broader training to CROs, including fire survival guidance refresher training. Given the endless cycle of faults, revisions and need for further training created by Vision, it is unsurprising that the Operational Support Team struggled to deliver fire survival guidance training.
Although it was obviously of the first importance that CROs should be able to mobilise appliances quickly, the LFB should not have allowed training on Vision to squeeze out other forms of training so completely during the four years between 2013 and 2017. For a number of years, but particularly in 2015 and 2016, the introduction of Vision was treated as a reason for ignoring or deferring essential training and even the reappraisal of training proposed by AC Chandler, despite the fact that the “Vision Training Plan” contemplated that training on handling fire survival guidance calls would take precedence and might cause delay to training on Vision.[1409] The failure of senior managers to ensure that training on fundamental skills required by CROs was maintained during that period reflects a failure to establish proper priorities and a weakness of organisation. When AC Brown was told that essential training was not taking place or had been severely curtailed, he should have required POM Hayward to ensure that the Operational Support Team provided essential training to the control room.
His failure to do so was particularly acute in the case of fire survival guidance training. Following the fire at Lakanal House and the LFB’s subsequent investigations, the importance of fire survival guidance training ought to have been clear to those responsible for the operation of the control room, including the Operational Support Team. It was a significant failure on the part of the LFB that fire survival guidance training was allowed to lapse during the introduction of Vision.
One longstanding problem affecting the control room was the perception that it was too difficult to arrange for CROs to undertake training while maintaining operational capability in the control room. A number of witnesses said that training on the watch was regularly interrupted by the need to recall staff to the control room to respond to incoming calls.[1410]
That was not a problem peculiar to the LFB or one which arose shortly before the fire at Grenfell Tower. The Fire Service Manual Volume 1: Fire Service Technology, Equipment and Media Communications and Mobilising, published in 1998, noted that training for control personnel had always been hindered by the small numbers of staff available and the need to maintain cover in the control room. Training was usually organised by watches and delivered at the place of work, thereby ensuring that the maximum number of personnel were available. Brigades were therefore advised to consider appointing a Training Officer and organising training days away from the control room.[1411] That document, published nearly 20 years before the Grenfell Tower fire, makes it clear that the difficulties posed by training at work were, or should have been, well known to fire and rescue authorities throughout the country. It is equally clear that it also proposed a solution to the problem.
In the Phase 1 report the chairman described the shift pattern operated by the control room, which was staffed by six watches. From the introduction of the new shift system in 2011 there had been a four-hour overlap between the early and late short shifts, which provided sufficient cover to enable training to take place during that period,[1412] but in 2014 the shift pattern had been altered, with the result that the short shifts overlapped by only two hours. It had been intended that staff on duty during one of the short shifts would undertake training during the hours with overlapping cover,[1413] but in his review AC George expressed the view that the shift pattern did not allow enough time for supervisors to provide regular effective training to their watches outside the control room.[1414] AC Brown had been heavily involved in consideration of the shift change in 2011 and had asked AC George to see how it could better accommodate training.[1415] In the report into his review AC George recommended that the control room should revert to the original shift pattern to allow four hours overlap between the short shifts that could be used for training.
Although the problem had been identified by AC George in 2016, the LFB had not tackled the reduction in the overlap between the two short shifts by the time of the Grenfell Tower fire. Indeed, it remained a contentious subject when AC Jonathan Smith produced his own review of the control room in 2019.[1416] He found even then that the use of the short shift was not providing the structured training that was required.[1417]
The importance of an adequate overlap between the two short shifts lay in the level of cover available for responding to the demands of the control room. In essence, the more staff present in the building, the lower the likelihood of the training watch needing to be called to control room duty.[1418] If there were a short increase in the number of calls to the control room, CROs could resume training, but if a significant incident occurred, a new date for their training had to be arranged by the Operational Support Team.[1419] The concern about the interruption of training is understandable, but to an extent misplaced. The evidence does not suggest that there was a frequent need to redeploy staff from training to the control room. On the contrary, POM Hayward said that it happened only infrequently[1420] and he was unable to recall being aware of any problems arising from the fact that staff were unable to complete their training because they had been recalled to the control room.[1421] There were other problems, however. For example, a shortage of staff in the control room meant that staff from the short shift were often needed to fill gaps in the duty watch.[1422] That inevitably reduced their availability for training.
As mentioned above, the Fire Service Manual recommended that brigades should consider appointing a Training Officer and arranging training days away from the control room.[1423] As a general rule, however, the LFB did not organise training “off-watch” or away from the control room.
It is clear from the evidence of control room staff that there was a commonly held belief that it was simply not possible to organise training “off-watch”. SOM Smith considered that the difficulty of making control room staff available for training at work was common to all fire and rescue services because it was not possible for them to go “off the run,”[1424] i.e. to be unavailable for duty. POM Hayward said that he had been unable to use overtime to provide training because he could not require staff to work overtime for that purpose and because he had already been making excessive use of overtime to maintain the necessary number of CROs on duty.[1425] However, in our view senior managers did not give sufficient consideration to delivering fire survival guidance training off-watch, given that in some other cases training was indeed delivered off-watch. For example, POM Hayward recalled that in August 2006, shortly after he had joined the LFB, staff had been trained on the ProCAD mobilising system off watch following a major revision.[1426] He thought that had been the only time staff had received training “off-watch”,[1427] but in 2010 the initial one-day fire survival guidance training had also been delivered “off-watch”.[1428] POM Hayward said that although at that time it had been possible to deliver training in that way, the introduction of the new shift patterns in 2011 and staff losses in 2012 had made training “off-watch” “problematic.”[1429] Despite that, SOM Smith told us that training “off-watch” had been provided in 2015 for the introduction of the new Vision mobilising system.[1430] CROs needed to receive a number of hours of training on Vision, which had been delivered to most of them “off-watch”.[1431] It is also the fact that in 2016 and 2017 some CROs worked overtime to support the command unit training exercises.[1432]
Those examples suggest that the belief that training could not be delivered “off-watch” was unjustified and unreasonable. They also suggest that fire survival guidance training was not considered by the LFB to be necessary to enable CROs to perform their role effectively. It is telling that although the introduction of Vision was considered to be of sufficient importance to justify “off-watch” training, the delivery of refresher fire survival guidance training was not. In view of the number of fire survival guidance calls the LFB had received during the Lakanal House fire and the lessons that it had itself identified, as well as the critical nature of the advice provided by CROs taking fire survival guidance calls, the failure to make any obvious effort to provide refresher fire survival guidance training “off-watch” was a serious error of judgment.
The shortage of staff to which POM Hayward referred had an obvious effect: in order to maintain the minimum number of staff in the control room, training would sometimes have to be cancelled.[1433] A shortage of staff, together with sickness and a need for breaks, was one reason why it had not been possible to train watches away from the control room during the short shift.[1434] However, the shortage of staff, its causes and consequences were well known. Between 2011 and 2012 the LFB was considering a proposal to enter into a contract with a third party for the provision of control room services, which resulted in a temporary halt to recruitment.[1435] That remained the position until 2016, when AC George asked for recruitment to resume after he had assumed responsibility for the control room.[1436] During his time as a director, AC George also increased the number of CROs and supervisors on each watch.[1437]
Following the Lakanal House fire, the Lakanal Control report identified serious deficiencies in the provision and recording of fire survival guidance training over the long period between 1981 and 2009.[1438] In his report following the audit of the training arrangements SM Kelly observed that, if fire survival guidance and other control room training were to be provided effectively, systems had to be established for planning training and recording its delivery.[1439] Yet, it is clear that, in the years following the Lakanal House fire, senior managers failed to establish such systems, so that the problems persisted up to, and indeed well beyond, 14 June 2017.[1440]
The need for fire survival guidance training to be structured and planned had been identified in FSC 10-93[1441] and in the Fire Service Manual published in 1998.[1442] Although national guidance was silent on keeping adequate records of training, the LFB’s own policy, PN164, issued on 29 September 1994 and amended on 28 January 2009, included detailed requirements on training records. In particular, paragraph 2.5 required a clear record to be kept of the contents of the training, together with details of dates, the trainers and any relevant notes,[1443] but it was not complied with. Moreover, PN164 did not require training plans to be produced for individual officers or watches or for the control room more generally.[1444] Those requirements ought to have been added to PN164 after the Lakanal House fire.
The LFB had originally intended that records of control room training should be brought into the StARS and STEP systems used by the rest of the brigade.[1445] In that way they would be automatically entered on STEP without the need for manual intervention[1446] and control room managers would easily be able to check what training each CRO had received and plan future training.[1447] The training records, as they existed at the time, were entered on STEP by 8 November 2010.[1448]
AC Brown accepted that, although he considered the biennial plan for fire survival guidance training to be robust, it did not amount to an all-encompassing training plan which met SM Kelly’s recommendation that an adequate system be introduced for planning training.[1449] However, neither he nor POM Hayward took any steps at the time to put such a plan in place.
At a Brigade Control Management meeting on 18 July 2012, AC Chandler discovered that there was no single document, such as a training matrix, which recorded what training had been delivered to control room staff and what was needed in the future. He therefore asked the OMs to collate that information for their own watches and present it in the form of spreadsheets. He also asked the Operational Support Team to produce a training matrix.[1450] It is clear, therefore, that SM Kelly’s recommendation to introduce an adequate system for planning training had still not been carried out almost two years after he had reported and that training records were still not being entered automatically on the StARS and STEP systems. It is also clear that after he became Head of Mobilising and Control in May 2012, AC Chandler recognised the importance of an effective system of planning training and took some steps to improve the position.[1451] POM Hayward could not explain why a training plan had not been established before July 2012.[1452]
At the meeting on 18 July 2012 OM Victor Bagnelle referred to the system of record-keeping introduced by the Operational Support Team as a temporary solution while adjustments were being made to the StARS and STEP systems to enable them to accept information relating to the control room.[1453] It involved recording information on a spreadsheet which was sent to the information management team once a month to be manually entered on STEP.[1454] The system was cumbersome and subject to human error, because different staff recorded training in different ways.[1455] Moreover, information about watch-based training was not always sent to the Operational Support Team for inclusion in the spreadsheet.[1456]
Training was discussed at the following Brigade Control Management meeting held on 12 September 2012, but no conclusion was reached.[1457] Obviously, therefore, no agreement had been reached on a training plan at that stage.[1458] AC Chandler recognised that the LFB would not have a robust defence if anything went wrong in the control room, but although another meeting was due to be held in October 2012 to discuss training,[1459] no training plan was in fact put in place.
In January 2013, GM Lindridge found that the control room was still recording all training on a spreadsheet to be entered on STEP manually.[1460] He also found that the technology made it impossible for control room managers to create a training plan on STEP and therefore recommended that a two-year rolling plan should be set out on a spreadsheet by January 2013.[1461] It is clear, therefore, that almost two and half years after SM Kelly’s report and six months after AC Chandler’s request for a training matrix, no training plan had been put in place and that StARS and STEP could still not be used to create training records for the control room.
POM Hayward could not explain why no training plan had been introduced by that point.[1462] Nor could he recall whether a training matrix had ever been produced.[1463] Apparently one reason why training records still had to be entered manually on StARS was because the programme still did not recognise the control room’s short shift patterns.[1464] He said that there had been competing priorities for attention, in the form of an amendment to StARS to accommodate a change in operational shifts and the introduction of Vision.[1465] He said that, because there had already existed a method of recording control room training, the necessary amendment had been moved down the list of priorities.[1466]
AC Brown agreed that there had been competing priorities, but he did not accept that operational demands routinely trumped the demands of the control room.[1467] He accepted that, although he had tried to push matters along, greater pressure could have been exerted to ensure that the control room’s training needs were given priority.[1468] He also suggested that the fact that the control room was based in Merton and was not a presence within the LFB’s headquarters probably made it difficult for its managers to make their case to senior officers.[1469]
On 4 April 2013, when AC Chandler returned from leave, AC Brown asked him to satisfy himself that the pre-inquest actions had been completed. He also asked AC Chandler to talk him through the training plan for the control room.[1470] AC Brown said that he had asked for that to be done because he remained dissatisfied with progress towards a training plan, which by then was overdue.[1471] He said that AC Chandler had told him that it was in hand.[1472] He also said that he had asked AC Chandler for the training matrix, but had not received it.[1473]
On 9 May 2013, POM Hayward sent an email to OM Victor Bagnelle expressing concern that the training database did not provide an accurate picture of the current state of training or the programme for future training.[1474] It is evident, therefore, that the planning of training was still not fully under control at that time. However, on 28 June 2013, AC Chandler reported to AC Brown on progress in completing the pre-inquest actions.[1475] In relation to action 16 he reported that the planning and recording of general control room training had improved.[1476] In light of the continuing problems with planning and recording training, the basis for that statement is unclear.
Very little happened until a year later, when on 22 July 2014, POM Hayward sent an email to SOM Bagnelle, SOM Diamond and SM Ajimal expressing concern at the absence of a robust system of recording control room training.[1477] His concerns were well-founded, and it is disquieting that in July 2014, although work had started, still no robust records existed and the objective of a training programme that was considered, planned and delivered to a measured outcome had not been met.
When SOM Smith took charge of the Operational Support Team and control room training in January 2015, she did not ask whether a training plan had been developed.[1478] She told us that POM Hayward had asked her to deliver a training plan for Vision.[1479] Although they had discussed delivering other training after Vision had been implemented, at that time attention was clearly concentrated on Vision.[1480] Accordingly, there had been a training plan for Vision but not for other training, such as training on handling fire survival guidance calls.[1481] SOM Smith told us that at that time the training plan had taken the form of large calendars displayed on a wall of the Operational Support Team’s office on which entries were made following discussions by email within the team.[1482] As she accepted, that did not constitute a detailed formally documented training plan.
In November 2014, the Directorate of Audit, Risk and Assurance in the Mayor’s Office for Policing and Crime audited the LFB’s arrangements for the management of the control room.[1483] It was the first time such an audit had been carried out.[1484] One of the matters that interested the auditor was how the training team ensured that all staff received fire survival guidance training annually.[1485]
The audit identified a number of risks, including:
It recommended that an independent record of fire survival guidance training be maintained and monitored for all control staff to ensure that all staff were in receipt of training at least annually and that a monthly report be produced by the Operational Support Team setting out the position in relation to training for the current year.[1487]
Both POM Hayward and AC Brown acknowledged that the risks identified in the audit had existed and that a failure to ensure that staff received adequate fire survival guidance training could result in serious injury or death,[1488] and we have no reason to think that they were not aware of those matters at the time. Yet, neither of them took effective steps to ensure that the auditor’s recommendations were implemented. AC Brown probably used the report as the basis for a discussion with POM Hayward to satisfy himself that everything was working correctly, but did not go further than that.[1489] It is unlikely that POM Hayward did anything beyond asking SOM Smith to check that the Operational Support Team was maintaining training records, because at that time they were concentrating entirely on training for the introduction of Vision.[1490] We do not consider that the drain on personnel resources caused by problems with Vision excuses the failure by senior management to give the auditor’s findings and recommendations the importance they deserved. That was a significant failure.
When he conducted his review of the control room in 2016 AC George found that training to maintain skills was irregular, not robustly planned and often not recorded on an individual’s training record. Staff often failed to record training and were seldom instructed to do so.[1491] He recommended that each OM ensure that an appropriate, robust, annual training plan was put in place for their own watch, agreed by their SOM and made available to all watch members and managers, and that training be recorded on an individual’s training record. He also recommended that senior managers should work with the LFB’s information management team to produce a solution similar to the training diaries used by station staff and make effective use of the brigade’s systems, including StARS.[1492]
SOM Smith was given the task of implementing AC George’s recommendations,[1493] although he accepted that he had been ultimately responsible for ensuring that that was done.[1494] He said that he had monitored progress through POM Hayward,[1495] but despite the force of his findings, StARS and STEP were not fully adapted to accommodate the control room until December 2018, nearly 18 months after the Grenfell Tower fire.[1496] It is also reasonably clear that although some work had been done, robust training plans for individual watches had not been put in place by the time of the fire.[1497]
The failure to adapt StARS and STEP to accommodate the control room was the root cause of the difficulties encountered with planning and recording training.[1498] AC George expressed surprise that previous managers had not made sure that the systems had been adapted to include the control room.[1499] Commissioner Dobson attributed the failure to a decision not to contract out the training of control room staff in 2012. He thought that, if that had been done, as it had for operational firefighters, the problems with training generally, and record-keeping in particular, would have been identified earlier. Regardless of the merits of Mr Dobson’s view, however, it is not a good excuse for the failure to plan, record and provide training after 2012.
When he carried out his review of the control room in July 2019, AC Jonathan Smith found that the current provision of training, assurance and professional development required a complete and systematic overhaul. Training was irregular and lacking in structure, there was no system of quality assurance and the recording of training was inconsistent. Those criticisms were linked to wider concerns relating to culture, accountability and leadership.[1500]
The failure to deliver regular fire survival guidance training after the Lakanal House fire represents a significant omission on the part of those responsible for the management of the control room. When senior officers were warned in the years after the Lakanal House fire that fire survival guidance training was not taking place, they should have taken effective action to make sure that it was provided. The management of fire survival guidance training was lacking in two other important respects: first, no objective criteria had been established by which to evaluate and monitor training or the quality of emergency call-handling; secondly, fire survival guidance training was not subject to consistent reporting or monitoring.
The LFB monitored only three aspects of the control room’s performance,[1501] all of which reflected performance indicators relating to the control room in the London Safety Plan.[1502] They were:
As far as the control room itself was concerned, it was for the AC and the POM to decide which aspects of performance should be monitored, but no discussion appears to have taken place between them about whether any other aspects of performance should be considered.[1504] That may have been because AC Brown thought that performance indicators were relevant only to things that can easily be measured.[1505] He thought that it was difficult to monitor quality because that required the evaluation of a process.[1506] There was no key performance indicator relating to training, although he took the view that, if the three indicators mentioned above were moving in the wrong direction, that would be a clear sign that training was not effective. For that reason, he thought that the three existing indicators provided some assurance that training was taking place.[1507] That was not the case, of course, because they related only to response times and did not reflect the content or quality of responses to calls, particularly fire survival guidance calls. It is, therefore, unreal to suggest that the key performance indicators could be treated as indicating the overall quality of training. It was a significant failure on the part of senior management not to recognise that there were no effective means of assessing the quality of responses to fire survival guidance calls.
AC George said that the three aspects of the control room’s performance to which we have referred reflected the information that LFEPA, as the LFB’s supervising authority, required.[1508] He thought that LFEPA was interested only in numbers and quantities, which effectively dictated their scope.[1509] Although he had reservations about that approach, there is no evidence that he or any other senior officer ever suggested that some other objective standard might be adopted by which to assess the quality of the control room’s responses to emergency calls generally or the quality of its responses to fire survival guidance calls in particular.[1510]
We referred earlier to POM Hayward’s laissez-faire style of management. He treated the absence of any reports of difficulties as an indication that the SOMs were managing training effectively, but the fact that fire survival guidance refresher training was not being consistently or effectively provided from 2012 onwards without his apparent knowledge demonstrates the weakness in his approach. There should have been a mechanism by which the SOMs or the Operational Support Team reported to him regularly about training generally and fire survival guidance training in particular. Together with a proper training plan and reliable training records that would have enabled him to monitor the provision of training against established criteria and satisfy himself and more senior managers that the LFB’s duty to train control room staff was being properly discharged.[1511]
It is significant that when AC Chandler was Head of Control and Mobilising, he recognised the need for improved arrangements for planning and recording control room training and was taking action to put them in place so that they could be easily audited.[1512] Some improvements had been made by June 2013,[1513] but it is clear that progress came to a halt when he left the LFB in October 2013,[1514] because, when AC George carried out his review in July 2016, he discovered that planning and recording training was still a problem.[1515] It is also clear that he did not address the problem effectively before he became Director of Operations in April 2017.[1516]
On any view, as AC Brown rightly accepted, the involvement of the assistant commissioner was important in the management of the control room.[1517] The consequences of leaving POM Hayward without effective supervision between October 2013 and March 2016 are clear from our description of how matters developed during that period.[1518]
AC Brown requested the appointment of an assistant commissioner to join the management of the control room as Head of Control and Mobilising in May 2012 precisely because he needed someone senior to manage it more closely than he could himself.[1519] He said that his position, which at that time was AC Operations, Prevention and Response and Third Officer, effectively combined two important functions, each previously performed by an assistant commissioner, with a significant increase in his responsibilities.[1520] POM Hayward said that as a result, his scheduled meetings with AC Brown would sometimes be cancelled or curtailed and he found it difficult to contact him.[1521] AC Brown accepted that, but said that meetings would be rearranged and that even if POM Hayward had not been able to get hold of him when he wanted to, there had been ample opportunity to discuss matters.[1522] He did accept, however, that when he had become Director of Operations in April 2015 the extent of his responsibilities had adversely affected his capacity to manage the control room generally and POM Hayward in particular.[1523] In an echo of AC George’s observation, AC Brown thought that the geographical separation of the control room had also contributed to difficulties in managing it, because when the control room had been moved to Merton, it had become both more difficult and more time-consuming to visit it.[1524] The net effect, according to POM Hayward, was that AC Brown did not actively supervise the management of control room training.[1525] POM Hayward made similar comments about AC Chandler and AC George, although it is evident that AC Chandler did exercise a greater degree of oversight.[1526]
AC Brown did not think it was his responsibility to examine the control room training records personally to ensure that fire survival guidance refresher training was being delivered properly. He relied on POM Hayward to schedule and monitor it and checked on the position at monthly management meetings. He could not remember having received any complaints about the response of CROs to fire survival guidance calls after the introduction of the regular training that followed the Lakanal House fire and therefore had not had any reason to question whether refresher training was taking place.[1527]
We accept that an officer of AC Brown’s seniority could not be expected to review details of training records personally, but the failures affecting the provision of training (and fire survival guidance training in particular) were longstanding and were well known to him and other senior officers responsible for the control room. As the various audits carried out between 2010 and 2016 consistently made clear, nothing effective had been done to remedy them. The responsibility for that failure must ultimately lie with AC Brown.
The criticisms of the way in which fire survival guidance calls were handled during the Lakanal House fire provided a powerful reason for senior management to satisfy themselves that fire survival guidance refresher training was taking place.[1528] Moreover, the discovery in February 2013 that the Operational Support Team had both reduced the time allocated for fire survival guidance training and removed the active role-play element[1529] should have sounded a clear warning that fire survival guidance training was not being provided as agreed in the wake of the Lakanal House fire. It should also have alerted him to the fact that positive action and close and regular scrutiny was required. In fact, although both POM Hayward and AC Brown demanded that fire survival guidance training be delivered as promised, neither of them did anything effective to ensure that it was.
The failure to provide the fire survival guidance training agreed by the Lakanal House Board should have prompted AC Brown to question the effectiveness of POM Hayward’s oversight of training, particularly given his more general concern about his day-to-day management of the control room.[1530] Although AC Brown said that he had raised his concerns with POM Hayward directly and had taken action to address them, POM Hayward said that the only concern that AC Brown had ever raised with him was that he did not communicate with him enough.[1531] Whatever the truth of the matter, the practical result was that AC Brown did not act on his concerns about POM Hayward’s management of fire survival guidance training. His failure to do so was serious, given the obvious risks to public safety.
The history of fire survival guidance training is long and complex, but the evidence gives rise to clear and consistent themes that reflect and confirm the broader failings of the LFB identified in this report. The control room was inadequately managed by POM Hayward who, in turn, was ineffectually led by senior managers, most notably AC Brown. The latter, in particular, was ultimately responsible for ensuring that CROs received the fire survival guidance training that they needed and also for ensuring that it reflected national guidance and the LFB’s experience at the Lakanal House fire. As is plain from what we have said above, AC Brown failed to do that, leaving CROs ill-prepared to meet the admittedly exceptional challenges of the Grenfell Tower fire.
In his Phase 1 report, the chairman found that from the earliest stages of the incident the deployment of firefighters inside the tower was hampered by generally ineffective communications, that communication difficulties significantly limited the efficiency of search and rescue operations[1532] and that it was well known within the LFB that BARIE sets performed badly in concrete high-rise buildings. He concluded that greater efforts should therefore have been made to establish and maintain effective communications inside the tower on the night.[1533] In this phase of the Inquiry we have examined the communication equipment used by the LFB in order to identify the source of the problems and have considered whether sufficient steps were taken to solve them.
A general description of the communication equipment used by the LFB on 14 June 2017 can be found in paragraphs 7.66–7.69 of the Phase 1 report, but for the purposes of this chapter it is necessary to describe it in a little more detail.
At the time of the Grenfell Tower fire the LFB relied on radio for communication between the control room and the fireground and between firefighters, both at the fireground and more widely. It used two kinds of radio equipment:[1534] ultra-high frequency (UHF) analogue radios and Airwave digital radios. (“Airwave” is the name of the network and of the network services provider.) In broad terms, UHF radios were used for localised, personal, operational use, principally on the fireground; Airwave radios were used for tactical functions, including communication with the control room and other emergency services.
The primary method of using UHF radio was by operation of a handset which acted as both transmitter and receiver. In addition, however, breathing apparatus radio interface equipment (BARIE) was used with the helmets and masks of many breathing apparatus sets.
UHF radio communications can be enhanced by radio repeaters, which receive and re-broadcast a radio signal, and by “leaky feeders”, which are cables that connect radio repeaters to form a series while simultaneously ‘leaking’ the radio signal to improve its reception between repeaters.[1535] Repeaters can be portable or fixed in buildings, tunnels and similar environments, or on LFB appliances.
Airwave digital radio, sometimes referred to within the LFB as the “main scheme radio”, was also mainly operated using handsets. In addition, however, all LFB appliances contained a fixed digital radio in the vehicle’s cab, which allowed crews to use the Airwave system to communicate with the control room and senior officers.
The central LFB policy on communications was Policy No 488 on Incident Communications.[1536] It set out the intended uses of each UHF channel as well as the responsibilities of a communications operator and command unit staff. A number of other policies that we do not need to mention here governed the deployment and use of specific items of communication equipment.
The LFB’s UHF radios had 10 channels, which were used for the following purposes:[1537]
UHF radios are intended for use locally, usually within the area of a particular incident. The signals travel a finite distance which, without interruption or interference, is determined primarily by the power of the transmitting handset.[1539] Professor Chris Johnson, a communications expert retained by the Inquiry, pointed out that the limited and localised range of UHF signals could be used to an organisation’s advantage by restricting the number of people who can receive a transmission to a localised team.[1540] However, that was not a relevant consideration in this case because of the almost complete loss of communications in the tower on the night of the fire.
The LFB’s handheld radios operated at a maximum power of 4 watts, but when transmitting on many channels were limited for historical reasons to 2.3 watts. BARIE sets, on the other hand, operated at only 1 watt. As a result, when crews were operating in the confines of a building, voice communications using BARIE sets might not reach their intended recipients without distortion or interference, or at all.[1541]
The LFB deliberately restricted the power of its BARIE sets to make them what is known as “intrinsically safe”, that is, of sufficiently low power to minimise the risk of creating a source of ignition when operating in a dangerous environment. Generally speaking, an increase in the power of a radio increases the risk of creating a source of ignition.[1542] For that reason, the LFB was reluctant to allow the use of more powerful radios in BARIE sets, particularly in environments that posed a risk of explosion, such as compartments or tunnels where gas might collect, and certain kinds of industrial premises. However, the need for intrinsic safety is less pressing in some circumstances, for example, when a fire has already started in a residential building. Although even in those circumstances there remains a risk that a radio might cause a gas explosion,[1543] the justification for not using intrinsically safe devices is that the risk is lower than in other environments in which flammable gas is likely to be encountered.
For similar reasons, the use of handheld radios by those wearing breathing apparatus was generally prohibited,[1544] but there were also practical reasons for not using them, principally the difficulty of operating them when wearing personal protective equipment. Nonetheless, the use of handheld radios was one way of trying to achieve better communications.[1545] It had therefore become common practice for firefighters wearing breathing apparatus to use their handheld radios without the incident commander’s approval and some certainly did so on 14 June 2017.[1546] As each team wearing breathing apparatus had only one BARIE set between them, one member of the team would be obliged to use a handheld radio if they became separated.[1547] There was also evidence that the earpieces in BARIE sets frequently became loose or dislodged, thereby preventing effective communication.[1548] In the event, therefore, BARIE sets were not a reliable means of communication in the difficult circumstances confronting firefighters in the tower.
As had become clear to the LFB during its investigations into the Lakanal House fire, the distance over which UHF signals travel is affected by surrounding objects and the built environment. It is common for nearby objects or materials to block, distort or reflect signals, thereby interfering with transmissions. That, in turn, can distort the message received by the recipient or block the signal entirely.[1549] As a result of the complex interactions between radio signals and objects in the built environment, Professor Johnson was unable to give a reliable estimate of the distance over which either the handheld radios or the BARIE sets would operate effectively in practice.[1550] However, he considered that the LFB’s estimated range of 500 metres or more using a 4 watt transmitter (assuming that the signals were unobstructed) was plausible.[1551] He was unable to estimate the range of signals transmitted at 1 watt (e.g., from a BARIE set), but was of the view that it would be significantly lower.[1552]
In fact, by 2017 it had been well known for some time that some kinds of construction materials (including metals, thick concrete, insulation, foil-backed materials and energy efficient windows) can interfere significantly with UHF radio signals, particularly if there is an accumulation of obstructions.[1553] As a result, UHF signals cannot travel to their full potential range between the floors of a high-rise building,[1554] given the distances involved, the materials used in their construction and other forms of obstruction. Those limitations are particularly important when considered against the backdrop of the limited transmission power of BARIE sets and the congestion in radio traffic caused by many users.[1555]
Congestion, which arises when more people attempt to use the system than it can handle at any one time, can affect both analogue and digital systems. In the case of an analogue system, only one person can transmit at a time,[1556] which means that firefighters need to wait for others to complete their transmissions before they can send their own messages. At a large incident there may be a lot of people waiting to send a message, which in turn can delay urgent or critical messages, as happened on 14 June 2017. If one person attempts to interrupt a message in the course of transmission that is likely to interfere with both signals.[1557] Those effects are likely to have been one cause of the communication difficulties experienced in and around the tower on 14 June 2017.
A rudimentary solution to the problem of congestion is to reduce the number of people using any given channel. That reduces the time a user has to wait for an opportunity to transmit, as well as the chances of users interrupting one another and causing signal interference. Using a larger number of channels for different groups of firefighters, or for specific activities,[1558] can go some way towards achieving that aim.
Radio signals can be enhanced by the use of portable radio repeaters and leaky feedercables but both pieces of equipment have a limited power to propagate signals and leaky feeders are typically effective only within sight of the cable,[1559] which significantly limits the value of deploying them in the stairwell of a high-rise building. Professor Johnson told us that he had seen no evidence to suggest that portable radio repeaters in combination with leaky feeders would restore communications in the majority of high-rise buildings in London.[1560] It should be noted that the Inquiry is not concerned with and has not considered the advantages of leaky feeders that are embedded within a building.
Commissioner Dobson and AC Reason said that the LFB resorted primarily to radio repeaters and leaky feeders as the fallback mechanism to combat difficulties with communications because they were understood to be effective and were the best solution available at the time of the Grenfell Tower fire.[1561] However, that approach failed to take account of the following points:
Although it was reasonable for the LFB to use radio repeaters and leaky feeders to alleviate difficulties with communications, given the limitations outlined above, it was not reasonable for it to rely on such equipment as its primary fallback mechanism for solving the problem of poor communications when operating in a high-rise residential building.
In Phase 1, there was evidence to suggest that at the Grenfell Tower fire digital radios had performed to a higher standard or provided better coverage than UHF radios. Digital devices essentially encode soundwaves into digital values and, in doing so, enable the signal to be encrypted.[1567] Digital radios can operate in two modes: direct mode (which is much like UHF radio in that the user communicates directly with another handset) and trunk mode, in which the radio transmission is sent via a base station, similar to a mobile telephone signal. When communicating in trunk mode, users join Airwave talk groups (equivalent to channels). The national Airwave network hosts a large number of talk groups; a document produced by the LFB in 2015 indicates that at that time it had access to about 70 talk groups but used only a handful at any given time.[1568] Because of their national coverage, talk groups can be assigned to a specific incident, location or activity, which provides an incident ground with more flexibility than the UHF system of separate channels.[1569]
Professor Johnson attributed the superior coverage of Airwave radios to their national, trunk mode operation,[1570] but it is important to note that, as in the case of analogue radio, digital radio signals are susceptible to blocking, degradation and interference.[1571] Although it is possible to enhance digital signals with repeaters,[1572] we have not seen any evidence that the LFB used, or contemplated using, such equipment in conjunction with digital radios.
Digital radios offer additional benefits, including the ability to compress data, enabling it to be transmitted using less bandwidth and thus reducing the chances of the network reaching the limit of its capacity.[1573] However, congestion can affect digital radios, although in a different way. Large numbers of people communicating over a talk group can result in Airwave reaching the limit of its capacity, which, in turn, prevents a signal from being transmitted.[1574] It follows that it is important to observe radio discipline, whichever technology is being used.
Most firefighters who attended the Grenfell Tower fire had only analogue radios (whether handheld or as part of a BARIE set). The LFB’s handheld digital radios were reserved for officers of the rank of station manager and above.[1575]
The use of handheld Airwave radios was subject to stringent security requirements due to their ability to gain access to encrypted radio channels used by the police and ambulance services and for reasons of cost.[1576] However, it is not clear that the security concerns surrounding the use of Airwave radios were insurmountable. The police and ambulance service use Airwave radios at all levels of seniority.[1577]
Even at the time of the Lakanal House fire in July 2009, the limitations of radio equipment of the kind used by the LFB were by no means unknown, having been demonstrated at several previous large-scale incidents.[1578] The following provide particularly clear examples.
The evidence showed that various people within the LFB held a substantial amount of technical knowledge about how construction materials of different kinds could attenuate or block radio signals,[1586] but that those who held that knowledge did not share it widely, with the result that the organisation as a whole did not make appropriate use of it. Although national guidance could have provided a clearer explanation of why high-rise buildings cause interference with radio signals, it did draw attention to the problem and recommend that fire and rescue services have contingency plans in place to ensure the safety of firefighters. For example, GRA 3.2, issued in February 2014, pointed out that high-rise buildings may cause difficulties with radio reception, including the creation of “blind spots”.[1587] The National Operational Guidance on Breathing Apparatus gave the same message when it warned that crews wearing breathing apparatus should be aware of the potential for limited penetration of radio signals through buildings and structures below ground and either make other arrangements or put contingency plans in place.[1588]
At the Lakanal House fire in July 2009, problems with the UHF radio signal made it difficult for the breathing apparatus entry control officer[1589] to communicate with crews relying on BARIE sets. Communications were also adversely affected by the volume of radio traffic at the incident.[1590]
Despite not being a new problem,[1591] the difficulties were serious enough to prompt the LFB to investigate their cause. The LFB’s Lakanal House Investigation Team, led by DAC Cutbill, was charged with that investigation. In April 2010, a radio expert, Roger Tuckley, produced a report for the LFB on the effect that steel-framed buildings can have on radio signals. It is unclear why the LFB focused attention on steel-framed buildings, since the purpose of the report was to provide answers to questions that might arise during the Lakanal House inquest.[1592]
Mr Tuckley’s report, a one-page note entitled “In Building Radio User Difficulties”,[1593] described a number of inherent restrictions affecting the use of UHF radio in the built environment, including the attenuating effect that buildings and objects within them can have on signal propagation. He also described the particular effects of certain construction materials, notably concrete, metal, solid foam insulation and insulation with foil backing. UHF radios operate best in situations where there is nothing between the transmitter and the receiver, which is typically not the case when they are used by BA crews. In view of its importance for understanding the performance of BARIE sets, the report was essential reading for the senior managers of the LFB’s operational departments. Despite that, it was not brought to the attention of AC Reason when he became Director of Operations, Resilience and Training in January 2012 or when he joined the Lakanal House Board in February 2012.[1594]
Despite the fact that Mr Tuckley had exposed significant limitations on the LFB’s UHF radios and had provided an explanation for the poor radio communications at the Lakanal House fire, the evidence suggests that little was done in response to his report beyond including it as an appendix to the LFB’s Lakanal House Operational Response Report.[1595] That report recorded only that most of the radios deployed at the Lakanal House fire had not been defective and that an unidentified report (which can only have been Mr Tuckley’s report) had advised that the height and construction of the building may have contributed to some of the comments made by crews. Mr Tuckley’s report did not prompt the LFB to consider how it might improve the resilience of its UHF radios or otherwise make up for their inherent limitations.
After the Lakanal House fire, the LFB’s Incident Communications department suggested that the power of handheld radios be reviewed and that the need for intrinsically safe radios in some circumstances be re-examined, but those suggestions were not passed to AC Reason[1596] and neither he nor Commissioner Dobson could recall having given them any detailed consideration when preparing the LFB’s response to the coroner’s rule 43 recommendations. They both said that the limited power of the BARIE radios reflected national guidance, from which the LFB was unlikely to depart.[1597] However, national guidance on breathing apparatus published by DCLG in January 2014[1598] had recommended that the level of intrinsic safety should be appropriate to the hazards likely to be encountered and should take account of other equipment being deployed by those wearing breathing apparatus. It also stated that electrical equipment other than that which was intrinsically safe might be considered appropriate for all normal operational requirements where it would confer a significant benefit to the safety and effectiveness of teams wearing breathing apparatus.[1599] We are not persuaded by Commissioner Dobson’s evidence that no steps were taken to implement that guidance because of disruption caused by industrial action. It was clear from his evidence that he was not familiar with it and there was no evidence within the LFB’s documents that it had been considered at all, let alone of any decision to delay its implementation between January 2014 and June 2017.[1600] In our view it is better understood as another example of the LFB’s reluctance to depart from established practices.
Improving radio communications was not one of the LFB’s pre-inquest action points (see Chapter 74). Commissioner Dobson could not account for that omission, but thought that it might have been because the problems with communications encountered at Lakanal House were not unusual and because advice had been received from technical experts that it was not possible to overcome some of them, given the circumstances in which radios were used.[1601] However, we have seen no evidence that the LFB’s senior officers were told that the problems were insurmountable, or that any consideration was given to whether they could be overcome or at least mitigated. Indeed, Commissioner Dobson’s evidence was that there was no review, let alone a root and branch review, of the existing technology following the Lakanal House fire.[1602]
We find that surprising. Given the importance of the observations made by Mr Tuckley, the LFB should have taken steps to investigate the practicability of mitigating or eliminating the problems he had identified. We have been left with the strong impression that the LFB viewed the kinds of communications difficulties experienced at the Lakanal House fire as an unavoidable incident of firefighting, particularly in modern high-rise buildings. A consequence of that attitude was that nothing was done between the Lakanal House fire in July 2009 and the Grenfell Tower fire in June 2017 properly to investigate the nature, extent and causes of those well-known difficulties to see whether it might be possible to mitigate or eliminate them. No satisfactory explanation has been offered for the LFB’s failure to pursue an enquiry into a matter of such importance to effective firefighting and the protection of crews.
In February 2013, during the course of the Lakanal House inquests, the LFB looked again at why its incident ground radios had not been wholly effective. DAC Cutbill asked GM A’Court (who was a member of the Incident Communications team) to consider the matter, but it is unclear why he did so, since, as DAC Cutbill knew, the LFB had already received detailed advice from Roger Tuckley which it had not taken seriously into account.
In his response dated 28 February 2013 GM A’Court explained once again that UHF radios work best in the absence of obstructions which reduce the propagation of signals and the distance over which they are effective.[1603] He explained that steel-framed buildings are more difficult for radio signals to penetrate than simple brick or timber-framed buildings and that the transmission strength of a signal has a bearing on its propagation. He described the signal strengths of the different channels used at incident grounds and noted that the transmission strength of BARIE radios was limited to 1 watt for safety reasons. Again, however, there was no evidence that anyone made use of that valuable description of the current equipment and the factors affecting its performance to consider the possibility of making changes to the LFB’s communications policies, equipment or practices. It is surprising, to say the least, that GM A’Court’s email was not brought to the attention of AC Reason, who by then was Director of Operational Resilience and Training.[1604]
At the conclusion of the Lakanal House inquests, the coroner recommended that the LFB consider whether it would be beneficial to use additional breathing apparatus radio communication channels and personal radio channels at major incidents to reduce the amount of traffic on each channel.[1605] In his response to the coroner of 23 May 2013 Commissioner Dobson explained that the LFB had considered doing so but had decided that using separate channels might make it difficult for crews to maintain an overview of an incident and might adversely affect operations, for example, by delaying the exchange of critical information and adversely affecting co-ordination between teams.[1606] The LFB concluded that the need to pass information across several channels might negate any apparent benefit because of the need to transmit the same information across all channels in use, thus reducing radio capacity and creating a risk of duplication and confusion.[1607] The Commissioner also said that the LFB had introduced breathing apparatus telemetry (a system which enables the entry control officer to monitor the air consumption of those wearing breathing apparatus),[1608] which reduced the amount of radio communication at incidents. He said that the LFB would ensure that the constraints on communication were covered in operational training, but he did not refer to the use of additional personal radio channels.
Responsibility for drafting the LFB’s response to the coroner’s recommendations on communications rested with the Incident Communications team, which was part of the Operational Policy department.[1609] The draft identified some potential improvements to communications which went beyond the coroner’s recommendation relating to the use of additional radio channels.[1610] The improvements suggested were sound and, if adopted, would have forestalled some of the concerns that have arisen during this Inquiry. They included:
For the sake of completeness, we note that an earlier draft of the document,[1611] which GM A’Court sent only to AC Knighton (then the Head of Operational Procedures)[1612] also suggested the following:
The Commissioner’s Group rejected the suggestions. Neither Commissioner Dobson nor AC Reason could remember why they had done so, beyond referring to a general (but not obviously well-founded) belief that the LFB’s systems were adequate.
Following the Grenfell Tower fire, the Operational Policy and Assurance department reviewed the specifications for fireground and breathing apparatus radios in advance of procuring new equipment. The review recommended that a single specification providing a transmitting power of 4 watts should be adopted for all UHF radios, but that a stock of radios with a higher intrinsic safety rating should be retained for specialist operational use.[1613] That approach could have been taken earlier in response to the national operational guidance on breathing apparatus issued by the DCLG in January 2014.
The LFB’s response to the coroner’s rule 43 letter was that it would ensure that the constraints on communications at incidents were covered in current operational training. In May 2013, however, the LFB provided very little training on the use of radio equipment beyond the initial training given to recruits as part of their firefighter development programme.[1614] The estimated completion date for the enhanced incident communications training was December 2013.
AC Reason said that he had understood that the new training would cover subjects such as using the correct equipment, using the correct channel, the availability of alternative channels, highlighting potential interference with the propagation of radio signals, the effect that certain kinds of buildings can have on the propagation of signals, options for circumventing problems and the equipment available for that purpose.[1615] The view within the LFB was that its communications procedures had broken down at Lakanal House because of the immense pressure under which firefighters were operating and that training might help to ensure that the procedures required to communicate more effectively were fixed in the minds of firefighters.[1616]
The process for commissioning that training was initiated by TCAP No. 0039,[1617] which was first issued on 27 July 2012, a date which indicates that the need for such training had been identified even before the Lakanal House inquests had begun. The training requirement was described in the form as being to ensure that all operational personnel had the knowledge and understanding required to use radio communication equipment in accordance with LFB policy to ensure effective communication at incidents.[1618] The final version, dated 10 March 2015, did not refer to the problems with communications experienced at Lakanal House or to the coroner’s recommendation. AC Reason said that he would have expected it to have done so, but plainly it did not.[1619] The absence of any reference to the LFB’s experience at the Lakanal House fire or to the coroner’s recommendation meant that the substance of the training programme was not informed by the matters it was intended to address. Once more, no senior LFB officer was able to explain that omission and there is no contemporaneous, or indeed any, document that explains it.
The resulting training packages were examined in detail during the oral evidence. Although the training package for station-based staff (that is, firefighters up to and including the rank of watch manager) described LFB radio equipment and radio enhancing equipment, it failed to explain how to use it or how to overcome communication failures. It did not explain the effect that the built environment can have on the propagation of radio signals, although that had emerged clearly from the Lakanal House fire and the LFB’s own investigations.[1620] Although the package for senior officers (station managers and above) provided more detailed information about the LFB’s radio equipment, it too failed to provide advice on how to overcome communications difficulties or information about the effect of the built environment on radio signals.[1621] Neither training package suggested the use of Airwave radios as a way of overcoming communication difficulties,[1622] nor did either of them distinguish between radio repeaters and telemetry repeaters, which became a source of confusion on the night of the Grenfell Tower fire.[1623] In short, the substance of the training packages did not adequately address the problems that had been clearly identified by both the LFB itself and the Lakanal House coroner. We have seen no evidence to suggest that anyone reviewed the content of the packages to see whether they covered those matters adequately.
However, the shortcomings of both training packages are completely overshadowed by the LFB’s failure to deliver them. Although they were approved, after some delay, in May 2015, they were not delivered to staff. The LFB attributed that failure to problems with its computer training system, which at many stations could not support training packages containing videos.[1624] However, only the package designed for senior officers contained video; the package designed for station-based crews was not affected by the limitations of the system. Peter Groves, the former Head of Development and Training, explained that a number of attempts had been made to solve the problem, none of which had been successful, and accepted that the videos could easily have been provided to stations by other means, such as CDs. That solution was apparently not considered, although it had been adopted for other training packages.[1625]
The story of communications is one of a succession of senior management failures to take active steps to improve what was known to be an unsatisfactory position. The rejection of GM A’Court’s proposals and the absence of any record of the reasons for rejecting them illustrate the LFB’s defeatist attitude towards the difficult task of providing effective communications. Our overriding impression is that the LFB’s senior officers saw the difficulties with communications as an intractable problem not amenable to any solution and for that reason nothing was ever done about them. However, given the obvious importance to firefighting operations of effective communications, such an attitude also suggests an unjustified complacency about the LFB’s ability to fulfil its role effectively without reliable communications.
The decision of the Commissioner’s Group not to adopt GM A’Court’s proposals is even more striking in the light of the publicity then being given to the problems with communications that had been encountered by the Hampshire Fire and Rescue Service during the Shirley Towers fire and were being investigated by the Hampshire coroner. The Hampshire Fire and Rescue Service’s report into that fire had been published on 8 April 2013, a few weeks before the Commissioner’s Group met in May 2013. It recorded that the handheld radios used by Hampshire Fire and Rescue Service did not always operate effectively in high-rise buildings and that the problem of poor radio communications in high-rise buildings was well known.[1626]
The report of the investigation into the Shirley Towers fire was released a week after the coroner at the Lakanal House inquests had made her rule 43 recommendations. AC Reason said that he had read the report when it was released and that it had been the subject of a report to the co-ordination board.[1627] In his evidence he agreed with the report’s conclusion that it had been well known that radio communications within high-rise structures could present problems, a matter of which the LFB had already been aware,[1628] but he had no clear recollection of the extent to which, if at all, the report had affected the LFB’s response to the coroner’s rule 43 recommendations.[1629] The LFB did produce a draft plan, dated 8 October 2012, for responding to various aspects of the operations at Shirley Towers, which included reviewing the meaning of a prolonged breakdown in radio communications referred to in materials such as procedures and training materials. The task was given to Operational Procedures,[1630] but we saw no evidence that any review had been carried out. AC Reason did not know whether any action had been taken in response.[1631]
The problems identified by the investigation into the Shirley Towers fire echoed problems which were well known to the LFB and the reaction of its senior officers reflected their defeatist response to the problems experienced during the Lakanal House fire. Although the causes of those problems had been identified by some within the organisation, the LFB failed to consider how best to address them. In essence, the Shirley Towers report did not prompt the LFB to reconsider its communications practices or policies, or, importantly, its response to the Lakanal House coroner’s recommendations on radio communications. As the Shirley Towers fire was yet another high-rise incident at which difficulties had been encountered using UHF radios, it should have elicited a more energetic response. Senior officers were unable to provide a satisfactory explanation for why nothing had been done.
In 2014, the LFB’s Operations, Resilience and Training Directorate had intended to replace the existing BARIE sets with more modern equipment, but the purchase of the new equipment was deferred because the current equipment was still available and was thought to operate effectively.[1632] That decision was unfortunate, given the wealth of evidence that many firefighters regarded the existing BARIE sets as unsatisfactory due to their limited range and the difficulties encountered in using them.
Apart from the BARIE sets, whose transmission power was limited to 1 watt, handheld radios could transmit at up to 4 watts. However, although channel 1 (the default incident command channel) operated at the full 4 watts, for historical reasons related to the previous generation of equipment, radios were set to transmit on other channels at 2.3 watts.[1633] Although that must have been known to some people in the LFB, by June 2017 no steps had been taken to increase the transmission power of handheld radios to 4 watts on all channels following the introduction of the current equipment in about 2007.[1634]
The story of TCAP No. 0039 is one of incompetence and inefficiency. The aim of the training packages was to address the kind of problems with communications that had been experienced at the Lakanal House fire, but their contents owed little to the LFB’s consideration of those problems or to the coroner’s recommendation and did not deal with them adequately. The LFB had access to three ‘spare’ UHF channels (channels 4, 7 and 8), but in June 2017 it was not its policy or practice to use them.[1635] The Incident Communications department drew attention to the possibility of using those additional channels,[1636] but senior officers decided against doing so, on the grounds that the benefits were likely to be outweighed by a lack of oversight of communications, a lack of co-ordination, and the possibility of delay in sending critical information.[1637] However, that reasoning is not consistent with the policy that firefighters wearing breathing apparatus should transfer from channel 6 to channel 5 if radio repeaters or leaky feeders have been deployed.[1638]
AC Reason told us that interference between channels had been a factor in the decision not to bring one of the available spare channels (channel 4) into regular use.[1639] Although that may be the case, we agree with Professor Johnson’s view that it might have been possible to persuade the government to reallocate the channels to maximise the use of the available frequencies.[1640] The fact that the LFB has brought some of those channels into regular use following the Grenfell Tower fire suggests that the problems of interference were not insurmountable.
An increased number of radio channels adds complexity to an incident and requires a robust system to ensure that the incident commander is made aware of all important communications. However, that should not represent an unduly onerous burden for a fire and rescue service responding to a large incident. A system of that kind is required at any incident where more than one radio channel is used, because an incident commander cannot be aware of all the communications generated, as LFB policy recognises.[1641] That complexity, and the potential need for a communications officer to oversee communications at larger incidents, will often be justified by the resilience that additional radio channels bring to fireground communications.
The LFB knew that the transmitting power of a radio and the surroundings in which it is being used both have a direct effect on the range of the signal. It should, therefore, have increased the transmitting power of handheld UHF radios and considered providing more powerful BARIE sets for use at residential fires, particularly those in high-rise buildings. A good start would have been to make a detailed assessment of the level of risk that wearers of breathing apparatus are exposed to using equipment with different levels of power, how frequently such risks arise, the effect of using more or less powerful radios and how the quality of communications could be improved in situations in which it was considered necessary for BARIE sets to remain intrinsically safe. AC Reason said that no such assessment had been carried out during his time.[1642]
The abundance of concrete, steel and more modern construction materials in Grenfell Tower is likely to have contributed to the significant deterioration of radio communications experienced by firefighters and officers in and around the tower on 14 June 2017. After the fire, the LFB tested radios at Grenfell Tower and found that they performed better than on the night of the fire. As a result, it attributed the problems it had experienced to congestion.[1643] We agree with Professor Johnson that that is an oversimplification.[1644] Although congestion is likely to have played a part in the failure of effective communications, we think it likely that the significant changes to the structure of the building brought about by the fire itself (including the destruction of most of the facade) explain most of the difference between the test results and the conditions experienced by firefighters on 14 June 2017.[1645] We also accept Professor Johnson’s opinion that signal propagation can be influenced by factors such as the weather and the presence of fire itself,[1646] and that those factors must also be borne in mind when considering the results of the LFB’s tests.
Notwithstanding its experience at the Lakanal House fire, the LFB did not teach firefighters or officers that the structure of a building and the materials from which it is made can interfere with radio signals, beyond giving them a broad indication that there can be blind spots within high-rise (or indeed other) buildings.[1647] More significantly, the LFB did not provide sufficient guidance to firefighters and incident commanders on how best to overcome difficulties with communications encountered in high-rise buildings. Such training may also have helped crews identify the risk of poor radio communications during section 7(2)(d) visits.
The LFB’s communications at the Grenfell Tower fire were generally ineffective.[1648] That was the result of many different failings and shortcomings, but in summary, the equipment deployed by the LFB on 14 June 2017 was inadequate, firefighters were not trained to identify and mitigate well-known and frequently encountered problems and LFB policies did not contemplate a widespread loss of communications or provide guidance on how they could be effectively restored.[1649]
Occasional failures of equipment are only to be expected and major incidents will always suffer from obstacles to consistently effective communications. However, that makes it all the more important to have contingency arrangements in place that can function cohesively to ensure the effective transmission of information. The LFB’s communication system on the night of the Grenfell Tower fire fell well short of achieving that objective.[1650]
In our view, the LFB’s approach to communications was to do the best it could with what it had available. As a result, it failed to make sufficient efforts to modernise its equipment and eliminate well-recognised defects in its systems.[1651] The LFB’s senior management concentrated almost exclusively on congestion as the primary cause of problems at large incidents, but for reasons given earlier, although a contributory factor, that was not the real difficulty. Senior managers appear to have accepted that communication problems were only to be expected and since little was done to challenge that conclusion and the suggestions made by the incident communications team were not implemented, no improvements were made. As a result, the LFB’s operational efficiency was significantly impaired.
The history of this matter neatly encapsulates the chronic defects in the LFB’s approach to well-known problems with incident ground communications. It consistently failed to accord to radio communications the significance and attention that they deserved, to address the problems that had been clearly identified and to train its personnel on how to deal with them when they arose. None of the senior officers who gave evidence was able to explain satisfactorily why the LFB had persistently failed to make a serious effort to solve problems which, although undoubtedly complex, were critically important for effective firefighting operations. For example, it is possible to set up a number of temporary Airwave talk groups for specific incidents or aspects of incidents, which is how the police and ambulance service use the system.[1652] There was no evidence to suggest that the LFB had considered using talk groups in that way, other than for training exercises, which may be a reflection of the limited number of officers who had personal Airwave radios. The broader adoption of digital radios (whether Airwave or otherwise), combined with the effective use of talk groups or channels, should have received more active consideration by the LFB before the Grenfell Tower fire. That might have improved the poor quality of communications inside the tower on 14 June 2017.
There were understandable concerns that there might have been a failure on the part of the utility company to make as much water available as possible on 14 June 2017 for firefighting purposes or a failure by the LFB to make the most effective use of the water that was available. We therefore considered it appropriate to investigate the supply and use of water in order to find out whether there had been any shortcomings and, if so, how they might be avoided in the future.
Fire and rescue authorities have a statutory duty to take all reasonable measures for securing that an adequate supply of water will be available for the authority’s use in the event of fire.[1653] If a fire and rescue authority asks for a greater supply and pressure of water than a water company would otherwise provide, the water company must take all necessary steps to comply and may shut off the water in any area to do so.[1654]
Due to the vast volume of water available in the Barrow Hill and Willesden reservoirs and accessible through the Thames Water Ring Main, there was more than enough water available to meet the demand for firefighting at Grenfell Tower.[1655]
The minimum water pressure in the network at the location of the hydrants used by the LFB was about 25 metres (2.5 bar),[1656] which exceeded both the minimum regulatory pressure of 7 metres (0.7 bar)[1657] and the 15 metres (1.5 bar) recommended by Ofwat.[1658] There is no minimum pressure requirement applicable to the provision of water for firefighting.
The water used for firefighting at Grenfell Tower was drawn from the general water distribution system, a complex network of pipes and valves used to transport water from storage (such as reservoirs and water towers) to customers and hydrants. The function of the water distribution network is to deliver an appropriate quantity and quality of water at a suitable pressure with minimal leakage, which it achieves using the force of gravity and the use of pumps.[1659]
Thames Water Utilities Limited (Thames Water) is the company which supplies water to London, including the Barrow Hill Zone in which Grenfell Tower is located. The Barrow Hill Zone is supplied by water from the Barrow Hill and Willesden reservoirs and has access to additional capacity provided by the Thames Water Ring Main.[1660]
When fire and rescue authorities require water for firefighting, they connect fire hoses to hydrants to deliver water to pump appliances, which in turn pump it through hoses to firefighting equipment.[1661]
The three most important factors affecting the supply of water from a distribution network to firefighting equipment are:[1662]
At the Grenfell Tower fire the LFB used fire hoses to draw water from the four hydrants shown in Figure 81.1 below: H1, a fire hydrant located to the south-east of the tower under Grenfell Walk,[1666] H3, a fire hydrant located at the intersection of Grenfell Road and Bomore Road,[1667] H8, a fire hydrant located on Bramley Road[1668] and H5, a wash-out hydrant located next to the Kensington Leisure Centre, which was wrongly labelled as a fire hydrant. (Wash-out hydrants are used by water companies for operational and maintenance purposes to flush out sediment and stagnant water, generally at significantly lower flow rates than fire hydrants. They are not designed to supply water for firefighting.)[1669]
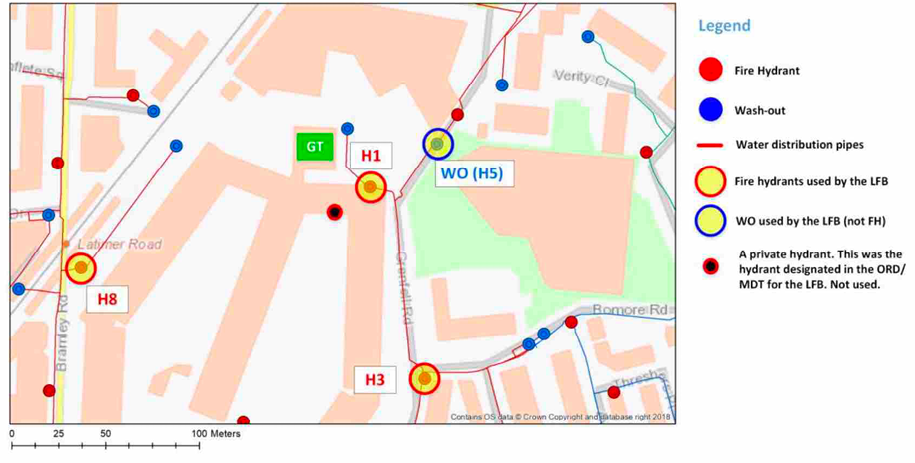
On 14 June 2017, between the first deployment of water at 01.15 and about 13.00,[1670] the LFB projected water on to the external face of the tower using aerial appliances, ground monitors and handheld branches.
Aerial appliances are fire engines with extendable ladders or cages from which water can be directed onto buildings.[1671] Three aerial appliances were deployed at Grenfell Tower: turntable ladder A213 TL (from 01.47 to 02.05),[1672] aerial ladder platform A245 (for less than a minute at 02.13, from 03.28 to 06.47 and from 07.14 to 09.45)[1673] and Surrey Fire and Rescue Service’s aerial ladder platform S13A1 (from 10.47 onwards).[1674]
Ground monitors are water nozzles which sit in a frame, enabling them to be placed on the ground and aimed in a particular direction without needing to be held by firefighters.[1675] Two ground monitors were used, albeit intermittently, at Grenfell Tower. One was sited on Grenfell Walk to the south-east of the tower (from 02.41 to 11.30)[1676] and another on the terrace of the Kensington Aldridge Academy to the north-west of the tower (from 02.43 to 10.52).[1677]
Branches are nozzles attached to fire hoses held by firefighters.[1678] Many handheld branches, including the first jet projected towards the window of Flat 16 from 01.15, were used at different times to project water onto the tower.[1679] Many were also used to extinguish burning debris on the ground surrounding the building.[1680]
Water for firefighting inside the tower was supplied through the building’s dry rising main from 01.06,[1681] and through an additional improvised fire hose into the south-west corner of the building from about 03.30.[1682]
None of the aerial appliances or ground monitors deployed at the incident was supplied at its maximum capacity due to restricted flow rates at the hydrants.[1683] That had three consequences.
In the light of the report produced for the Inquiry by Dr Stoianov, the LFB carried out a series of tests to determine the maximum height of the jet that could be practically achieved by aerial appliances and ground monitors of the kind used at Grenfell Tower.[1690] The maximum heights achieved during the tests were (with one exception) higher than those achieved on 14 June 2017, but not high enough to reach the top of the tower.[1691] In his supplementary report[1692] and oral evidence to the Inquiry,[1693] Dr Stoianov made strong, and in our view, persuasive, criticisms of the testing method used by the LFB, most significantly, that it had failed to supply the appliances with water at their maximum rated flow rates or pressures. For that reason, he did not accept its conclusion that the aerial appliances were unable to project a water jet to a height of 65 metres.
Although Dr Stoianov’s calculations provide some helpful indication of the maximum height that aerial appliances could reach in optimal conditions, he rightly accepted that there were matters beyond his knowledge and expertise that could limit the height to which a water jet could be projected in practice. They included weather conditions,[1694] the performance of pump appliances[1695] and, most significantly, operational factors affecting the use, siting or angle of the jet.[1696] Examples include obstructions impeding the siting of appliances, including burning debris falling from a building,[1697] and a possible reduction in the firefighting effectiveness of a jet when operated at the limit of its vertical reach.[1698]
For these reasons, we cannot safely make any finding about the height to which aerial appliances might have been able to project water on 14 June 2017 if they had been supplied at their maximum rated flow and pressure. However, we have no hesitation in accepting Dr Stoianov’s opinion that the height of the jets produced by the aerial appliances at Grenfell Tower was limited by the low flow rates at which water was supplied to the pump appliances.
An example of periodic interruptions in the use of equipment caused by low flow rates can be seen in the operation of appliance A213 from 01.47 to 02.05. The tank of the pump appliance supplying it repeatedly became empty after less than a minute, requiring A213’s water jet to be interrupted for about 20 seconds to allow the tank to refill before it could be started again. Firefighter Raymond Keane improvised a partial solution by turning down the settings of the pump supplying A213, resulting in a continuous, but less powerful, jet.[1699] Similarly, the initial operation of appliance A245 at 02.13 lasted for only 47 seconds until the tank of the pump supplying it became empty.[1700] The same problem affected the ground monitor on Grenfell Walk and aerial ladder platform S13A1, resulting in repeated stoppages throughout their operation.[1701]
Aerial ladder platform A245 was one piece of equipment that could not be deployed as originally intended. Following its redeployment at 03.28, the flow rate delivered to A245 was too low to enable its monitor to be used effectively. Firefighters therefore improvised by strapping a smaller 22 mm high-pressure hose to the cage of A245 to produce a jet which could reach the tower,[1702] the equivalent of pinching the opening of a garden hose to produce a longer but narrower stream of water.[1703] Similarly, the flow rate delivered to S13A1 was insufficient to make use of its built-in monitor without interruption and firefighters tried using a smaller diameter hose to produce a jet that could reach the tower. However, that was unsuccessful and they reverted to using the monitor of S13A1 for 20 seconds and then waiting about a minute for the tank of the pump supplying it to refill.[1704]
One significant factor contributing to the low flow rates delivered at the outlets was a loss of pressure in the hoses between the hydrants and the pump appliances.[1705] Some pressure loss is unavoidable, but on the night of the fire this was exacerbated by the long distance from the hydrants to the tower (about 95 metres and 125 metres for hydrants H3 and H8 respectively). Those losses were partially redressed by using pumps in relays (i.e. two pump appliances deployed in series) for hydrant H8 and, from about 06.00 onwards, for hydrant H3.[1706] The main cause of the problem, however, was the low flow rates delivered by the hydrants themselves,[1707] which were caused principally by the following three factors:[1708]
Water companies have a statutory duty to keep all fire hydrants attached to their pipes in good working order and to replace any hydrant when necessary.[1709] British Standard 750:2012[1710] (BS 750) states that fire hydrants should have a flow coefficient of not less than 92.[1711] BS 750 does not state whether that relates to a simple hydrant tested under factory conditions or to a hydrant installed in the pipework necessary to connect it to the water network. The distinction is relevant because the flow coefficient of a hydrant installed in a pipework system will necessarily be lower than (or, at best, equal to) that of a simple hydrant due to pressure losses introduced by the connecting pipework.[1712]
Paragraph 10.2 of BS 750 requires the flow coefficient of a fire hydrant to be specified in the manufacturer’s literature. If the flow coefficient of a hydrant installed in a pipework system may be affected by pressure losses introduced by the particular characteristics of the connecting pipework, as Dr Stoianov told us was the case, its performance in service will, or may, depend to some extent on the system into which it has been incorporated, which is inherently variable and not something of which the manufacturer could be aware. We therefore think that the requirement in BS 750 must be understood as relating to the hydrant tested under factory conditions. However, it would avoid confusion if the British Standards Institution were to make the position clear.
Testing carried out by Dr Stoianov showed that the flow coefficients of the fire hydrants used at Grenfell Tower ranged between 31 and 74.[1713] As the hydrants were installed in the network, he was unable to test their factory standard flow coefficients. We have not had access to the manufacturers’ literature relating to those hydrants and do not know whether their flow coefficients under factory conditions were 92, as required to conform to BS 750. However, Dr Stoianov told us that he would expect the installation of hydrants to be carried out in such a way as to maximise their flow coefficients and that he would have expected the flow coefficients of the hydrants used at the Grenfell Tower fire to be higher.[1714] If that had been the case, they would have provided greater flow rates to firefighting appliances and equipment.
Hydrant H5, which was used to supply aerial appliances A245 and S13A1, is not a fire hydrant but a wash-out hydrant, which is not designed to supply water for firefighting. It had a flow coefficient of 31, lower than the flow coefficients of the other three hydrants used at the Grenfell Tower fire, which ranged between 50 and 74.[1715] Hydrant H5 had been wrongly labelled as a fire hydrant. The labelling of the hydrant was the responsibility of Thames Water.[1716]
On 14 June 2017, neither the LFB nor Thames Water realised that H5 was a wash-out hydrant, although its status was indicated on Thames Water’s Geographical Information System,[1717] to which its technicians and the staff of its Network Management Centre referred during the incident.[1718] Having been mislabelled as a fire hydrant, there was no practical way for firefighters to tell that H5 was in fact a wash-out hydrant.[1719]
In his evidence to the Inquiry, Dr Stoianov said that he had notified Thames Water of the mislabelling of H5 while undertaking hydraulic testing in 2018.[1720] At some point between September 2018 and July 2019, Thames Water then replaced the metal frame of the wash-out chamber and the metal lid of H5 with a correctly labelled “W” plate.[1721]
The LFB contacted Thames Water’s Network Management Centre by telephone at 01.28 on 14 June 2022 to ask for the attendance of a water technician and an increase in the water pressure.[1722] Two water technicians attended the incident at 02.15 and two more at 04.15, followed by two more at approximately 07.30. After the initial call and subsequent confirmation from Thames Water that technicians were on their way, there was no further direct contact between the LFB’s control room and Thames Water. Communications between the LFB and Thames Water took place between firefighters and water technicians at the incident ground. They included two requests from the LFB to increase the supply of water, one from WM Beale at about 02.30 and one from SM Payton at about 10.05.[1723]
Thames Water made two changes to the water distribution network in an attempt to increase the amount of water available for firefighting. Technicians opened two boundary valves, at 03.09[1724] and 11.05[1725] respectively, with the aim of increasing the water pressure in the area around Grenfell Tower by connecting it to different parts of the water network and so spreading any pressure losses across a larger area.[1726] However, that did not significantly increase the pressure at the hydrants being used by the LFB. It therefore had no significant effect on the flow rate at those hydrants[1727] and caused no material improvement in the supply of water to the firefighting equipment.[1728]
Technicians from Thames Water also provided assistance at the incident ground. Between 06.00 and 06.30 they helped to clear blocked drains that were causing flooding around the tower and hindering firefighters’ access to the building. At approximately 06.30, a technician opened fully the valve on a hydrant which had previously been only partially opened, resulting in an increased flow.[1729]
Water companies commonly use pressure reduction valves at certain points in the network to minimise water leaks and burst pipes, which are more likely to occur at higher pressures.[1730] During normal operations in June 2017, Thames Water operated a pressure reduction scheme in the Grenfell Tower area, which was implemented by the use of pressure reduction valves which it could operate remotely.[1731] On 14 June 2017, the pressure reduction valves remained open throughout the incident, which Dr Stoianov estimated resulted in a reduction in water pressure of between 0.7 and 1.3 bar.[1732] At 03.55, the Thames Water’s Network Management Centre told the technicians at the incident how to switch off the pressure reduction valves, but the technicians decided against doing so because they were concerned that if the pressure became too high it might burst the pipes, a decision with which the Network Management Centre appears to have agreed.[1733] If a pipe had broken, it could have led to the loss of a substantial amount of water and a widespread loss of pressure, putting the entire water supply to Grenfell Tower at risk.[1734]
We think it likely in the light of Dr Stoianov’s evidence that the pressure reduction system could have been switched off to produce an increase in water pressure of 0.7 to 1.3 bar, with only a minimal risk of a broken pipe,[1735] although that would have provided only a modest increase in the flow rate from the hydrants of between about 180 and 420 l/min.[1736] A single handheld firefighting branch requires a flow rate of 400 l/min.
Another feature of the day-to-day operation of the water distribution system at Grenfell Tower was the automatic cycle of the Hammersmith pumping station. The Hammersmith pumps operated to increase water pressure in the area during the day, when demand from customers was higher, and were automatically switched off between 00.30 and 05.30, when demand was lower. On 14 June 2017, the pumps operated as normal.[1737] At 02.59, Thames Water appears to have decided against switching on the pumping station, again due to the risk of bursting a pipe.[1738] In the light of Dr Stoianov’s evidence we think that the Hammersmith pumps could have been switched on before 05.30 to increase the pressure available in the network with a minimal risk of breaking a pipe,[1739] but again, that would have provided an increase in the flow rate at the hydrants of only about two to three litres per minute.[1740] Given the scale and intensity of the fire, it is difficult to see that that would have made any significant difference to the LFB’s firefighting efforts.
We should note that Dr Stoianov was critical of the level of technical and engineering support provided by the Thames Water’s Network Management Centre during the incident. In particular, he thought that better use of available data, modelling and information about the network might have allowed it to recommend more efficient arrangements for the supply of water.[1741] However, it seems unlikely that they would have secured a significantly greater supply.
Dr Stoianov drew our attention to several misunderstandings and incorrect assumptions made by firefighters and Thames Water personnel on 14 June 2017 about the water network. Most notably, they included:
The operational firefighting response to the Grenfell Tower fire was investigated in Phase 1. In this chapter we address two particular topics relating to operational firefighting which the chairman considered called for further consideration in Phase 2:
In the Phase 1 report the chairman made findings about the deployment of the principal items of equipment used by the LFB as part of its operational response to the fire. They included findings, to the extent that the evidence allowed, about the times and locations at which equipment was used during the course of the incident. In Phase 2, we have considered the effectiveness of that equipment and its deployment on the night of the fire, as contemplated in the Phase 1 report.[1745]
The aerial ladder platform brought to the incident by Surrey Fire and Rescue Service (S13A1) could deploy water from a height of 42 metres, in contrast to similar vehicles operated by the LFB, which could project water from a maximum height of 32 metres.[1746] Given that S13A1 was not used until after the last casualty had been rescued, the effectiveness of that aerial appliance has not been considered as part of our investigations.
In Mr McGuirk’s opinion the LFB was successful in applying water to all four sides of the building, based on his own appraisal of the contemporaneous evidence and Dr Barbara Lane’s analysis of the extent to which fire spread over the external walls on each side of the tower.[1747] The available images show a clear inverse correlation between the deployment of external firefighting equipment and the downward spread of fire, which was more limited on the south and east faces of the tower (down to floors 10 and 18 respectively) than it was on the north and west faces (down to floors 9 and 7 respectively). The images also show that a higher reach was achieved by the equipment deployed against the south and east faces of the tower, namely the ground monitor on the south side walkway and aerial ladder A245 on the east side. A213 contributed to the external firefighting on the east side, but to a much more limited degree, given the relatively early stage at which it needed to be moved away from the tower.
It is clear that water was applied to the external faces of the north and west sides of the tower, albeit to a lower height, either by ground monitors or handheld jets or, more likely, a combination of the two, and appears to have been effective in limiting the downward spread of fire. That is consistent with Dr Stoianov’s assessment of the application of water to the tower over the course of the incident.[1748]
It is indisputable that the operators of the two aerial appliances on the east side of the tower, CM Daniel Harriman and FF Christopher Reynolds (who were in charge of A213) and CM Christopher Frost and FF Jason King (who were in charge of A245, overseen by WM Stuart Beale), demonstrated considerable courage and ingenuity on the night of 14 June 2017. CM Harriman and FF Reynolds operated their appliance for as long as practicable in very difficult circumstances, putting their own safety at risk from the burning debris that began falling from the tower soon after the appliance had been set up. CM Frost and FF King were successful in setting up A245 on the grass by the tower, although that was not in accordance with established procedure.[1749] As Mr McGuirk said, that was a calculated risk and an appropriate exercise of initiative.[1750] CM Frost and FF King, overseen by WM Beale, also successfully devised a system that enabled their aerial to apply water up to floor 13 of the tower by strapping a high-pressure hose on to the cage of the platform.[1751] That measure ensured an effective supply of water at the top of the appliance, despite the problems that the crew had initially experienced when trying to operate the monitor built into the cage of A245.[1752] That was pure improvisation on the crew’s part and, again, it was an appropriate and considered use of initiative, which assisted in the external firefighting efforts on the east side of the tower.
Taking all that into account, the LFB personnel who were responsible for external firefighting acted diligently and professionally in extremely difficult circumstances, including the fact that the ability of each of the aerial appliances to project water was limited primarily by the low water flow provided by the hydrants. That was particularly so in relation to A245, the water for which was supplied by the incorrectly labelled wash-out hydrant.[1753] To a great extent, those factors were outside the control of the LFB personnel managing the appliances. It was not the LFB’s responsibility to ensure that hydrants were correctly labelled[1754] and we therefore make no criticism of the firefighters who used that hydrant.
There are, however, two points that should be made. First, it is unfortunate that the information on the Mobile Data Terminal about the location and operational status of hydrants in the vicinity of Grenfell Tower was inaccurate. Hydrant H1, which was used to supply appliance G272, was not identified at all and Hydrant H4 was incorrectly labelled as defective,[1755] but it is unlikely that those inaccuracies made any material difference to the effectiveness of the operational response. However, it is yet further evidence of more general problems with the LFB’s systems for the collection and management of operational risk information.
Secondly, we agree with Dr Stoianov’s view that the communications between firefighters on the incident ground and Thames Water’s technicians, who relayed information to the Network Management Centre,[1756] were essentially casual in nature causing relevant information to be lost or not communicated at all. We recognise that the firefighters who spoke to Thames Water either in person or by telephone were operating under enormous pressure and were doing their best to improve the effectiveness of the equipment being used. Nonetheless, there is no record of any clear and explicit request having been received by the Network Management Centre to make water available in accordance with the requirements of the main appliances in use at the incident.[1757] WM Beale said that he had asked one of the technicians on the incident ground for more water, but in the absence of any formal or consistent system for passing requests to Thames Water, it is not surprising that the request was not received or formally noted at the Network Management Centre.[1758] In any event, it was not the responsibility of operational personnel, who were trying to carry out or oversee firefighting operations, to ensure that the specific requirements of those appliances were communicated to the Network Management Centre. In the first instance, that should have been the responsibility of a bulk media adviser.
Subject to those qualifications, the firefighters involved in the firefighting operations outside the tower did all that they reasonably could to extinguish the fire and to protect the lives of those inside the building.
Positive Pressure Ventilation fans (PPVs) provide forced ventilation which can be used to clear smoke-filled environments or to prevent smoke from entering a clear space. The fan increases the pressure of the air in the area in which it is placed, thereby causing air to flow into the adjacent space. The technique is commonly used in multi-storey buildings.[1759]
At the Grenfell Tower fire a PPV fan was requested at 02.57 and again at 03.07. Two PPV fans arrived at the incident ground at about 04.00 and were used for a very short time in the lobby of the tower, before being stopped because they were increasing, rather than reducing, the amount of smoke in the lobby.[1760]
Mr McGuirk explained that, when fighting a fire in a high-rise residential building, a PPV fan needs to be sited in the first instance at the entrance to the stairwell where it can direct fresh air into the stairwell to clear it of smoke.[1761] There may be an opening at the top of the stairwell through which air and smoke can escape, but fans can still be deployed effectively even if there is no opening.[1762]
It is clear that PPV fans could not have been used effectively at the Grenfell Tower fire, primarily because of the layout of the ground and mezzanine floors. For example, positioning them in the lobby area on the ground floor, as was done, would only have pressurised that area because of the door that led to the stairwell on the mezzanine on floor 2. They could have been moved into the stairwell, but would then have been able to draw air only from within and not from outside the building. The effect would have been to recirculate the smoke that was already in the stairwell,[1763] which was precisely the problem encountered by the firefighters who tried to use them. It is highly unlikely, therefore, that the fans that were brought to the tower could ever have reduced the spread of smoke within the stairwell or anywhere else in the building outside the lobby area.
A light portable pump is a small, purpose-built, petrol-powered pump capable of providing a water supply from sources that are not accessible to standard pump appliances (for example, a lake). Pumps of that kind are normally used in rural locations and are designed to deliver small quantities of water. They have a limited pumping capacity of no more than 1,000 litres per minute and can produce relatively limited pressure. They require regular refuelling and, because they emit exhaust fumes, are suitable for use in the open air rather than inside buildings.[1764]
There is some evidence that a light portable pump was brought to Grenfell Tower in the later stages of the incident, but it is unclear whether it was used.[1765] It is unlikely, however, to have made any material difference to the supply of water or indeed the operations that the LFB was able to carry out inside or outside the tower. In particular, the limited pumping capacity and pressure achievable by a pump of that kind meant that it was not capable of providing any significant increase in the supply of water for firefighting. It would also have been unsuitable for use inside a residential high-rise block due to the emission of exhaust fumes.
The Inquiry heard evidence in Phase 1 about two other pieces of equipment that were potentially available, but which were not used at Grenfell Tower: smoke hoods and smoke curtains.
Smoke hoods are used to protect members of the public from smoke and noxious fumes for a limited period while they are being helped by firefighters to leave the building.[1766] Smoke hoods were not commonly used before the Grenfell Tower fire, but they have since been adopted by a number of fire and rescue services, including the LFB and Kent Fire and Rescue Service.[1767]
We think that smoke hoods could certainly have helped in the rescue of some residents of the tower, as is illustrated by the rescue by CM Tillotson’s crew of two residents from floor 9 of the tower with the aid of two additional breathing apparatus sets that they had collected from the bridgehead to be worn by the residents as they were helped out of the building.[1768]
Smoke curtains are sheets of fire-resistant material attached to a frame that is designed to be inserted into an existing door frame. A small opening in the base of the curtain allows firefighters to pass in and out through the door, while preventing or minimising the passage of smoke.[1769] The function of the curtain is to protect the integrity of the smoke-free area on the other side (typically the stairwell) while allowing firefighters to enter the smoke-filled area to carry out firefighting or search and rescue operations.
Like smoke hoods, smoke curtains were not commonly used before the Grenfell Tower fire but have since been introduced by a number of fire and rescue services,[1770] including the LFB.
Smoke curtains may be a useful way of preventing or minimising the spread of smoke within a building where there has not been widespread compartmentation failure. We think they could have been used in the first hour or so of the incident to reduce the amount of smoke entering the stairwell and thereby help residents escape. However, we do not think they would have been likely to help much after that time because of the extent to which the smoke had spread and the number of compartmentation failures.
In the Phase 1 report the chairman recognised that the firefighters who attended the Grenfell Tower fire displayed enormous courage and selfless devotion to duty.[1771] We echo that finding, but their bravery and commitment to duty is only a part (albeit a significant part) of the picture. Another part is the inescapable fact that the systemic failings of the LFB on the night of the Grenfell Tower fire relating to training, incident command, communications and the operation of the control room had all been foreshadowed by previous fires, most particularly, the Lakanal House fire on 3 July 2009.
The LFB did not fail to identify or understand the lessons to be learnt from the Lakanal House fire and other major fires involving high-rise buildings constructed using modern materials and methods of construction. On the contrary, its response to the Lakanal House fire in particular showed that it understood its significance immediately. The LFB quickly analysed the incident and identified the appropriate lessons including the broader implications of the increasing use of modern materials and their role in promoting external fire spread. In that regard, Commissioner Dobson’s correspondence with DCLG in December 2012 showed commendable foresight in anticipating many of the questions that have been investigated in Phase 2.
The LFB’s failure lay in its inability to implement any effective response. That failure had many causes, but it is possible to identify in the evidence summarised in previous chapters a number of distinct but closely related aspects of the way in which the LFB was managed which, in our view, account for it. The evidence clearly shows that the LFB’s failure was attributable to a chronic lack of effective leadership, combined with an undue emphasis on process and a culture of complacency. Senior officers appear to have thought that establishing bodies to review and report would inevitably lead to action without the need for effective monitoring of progress and further action being taken as necessary to ensure completion. Complacency led to a failure to ensure that knowledge of the dangers presented by the increasing use of combustible materials were reflected in operational policies and procedures.
Ron Dobson and Dany Cotton, as former Commissioners, bear ultimate responsibility for the LFB’s inability to take effective action after the Lakanal House fire. It is to their credit that neither of them shirked nor sought to qualify that responsibility. However, their acknowledgment should not obscure the failures of other senior officers who were directly responsible for the efficiency and effectiveness of their departments. In the decade before the Grenfell Tower fire, Dave Brown, as Third Officer and Director of Operations, oversaw a broad range of the LFB’s activities which have featured heavily in Phase 2.
Two failings, in particular, illustrate AC Brown’s approach to command and management and explain in part why recommendations were not carried out effectively. The first concerns the inspection of high-risk high-rise residential buildings. That function was (and remains) a necessary and important means of making sure that the LFB discharges its duties under the 2004 Act and the Health and Safety at Work Act 1974. AC Brown did not wish to become involved in considering the complexities of an inspection regime, a problem which deserved more careful consideration than he was willing or able to give it. If the letter and spirit of the Lakanal House coroner’s recommendation were to be met and more effective inspection arrangements introduced, GM Elwell’s recommendations required proper consideration. AC Brown failed to give them that consideration and, as far as we can see, there was no good reason for that. If those proposals had been implemented, they could have gone some way towards remedying the deficiencies in the LFB’s arrangements for gathering and managing operational risk information.
The second example relates to the control room. The importance of fire survival guidance refresher training for CROs is obvious. The senior officers responsible for the control room (including AC Brown and POM Hayward) plainly understood that importance, particularly because of the weaknesses in handling calls exposed by the Lakanal House fire. In 2009, no structured or regular fire survival guidance refresher training was provided by the LFB and this was still the case at the time of the Grenfell Tower fire in 2017. The failure to give CROs regular fire survival guidance refresher training is a serious shortcoming, particularly by those officers who were responsible for making sure that effective training was provided. Even allowing for the difficulties flowing from the introduction of Vision, there is no justification for such a longstanding failure to address a vital element of the control room’s work and one which touched directly upon public safety.
An aggravating feature is that even though the Lakanal House fire demonstrated the real danger to life posed by the failure to provide effective fire survival guidance training, none of senior officers responsible for the operation of the control room ever tackled the challenge of providing the necessary training with the dedication it deserved.
Although individuals undoubtedly had a role in the failings which have been examined here, it is important to stress that they were committed in the context of broader structural and cultural problems. It is clear that the LFB’s response to the Lakanal House fire placed undue reliance on process. Boards were established, plans were made and reviews were commissioned, but no effective steps were taken to ensure that recommendations had been effectively implemented, particularly in relation to the danger of relying uncritically on compartmentation, the risk of fire spreading across external walls and the ability to handle many fire survival guidance calls simultaneously. Because those matters were not addressed in the resulting training packages, the recommendations were not fully implemented and so the defects that had been identified were not remedied.
The root cause of the problem was that the LFB’s senior officers lacked the necessary degree of managerial competence to recognise and correct problems. One stark illustration of that shortcoming is the failure to translate its longstanding knowledge of the dangers posed by modern materials and methods of construction into operational policies that recognised and reflected those dangers. Another is the failure to ensure effective management of the control room, particularly in relation to training. Commissioner Dobson was alert to the danger posed by the use of combustible materials and in December 2012 recommended certain measures to DCLG that might have alleviated it. However, in the eight years between the Lakanal House fire and the Grenfell Tower fire neither he nor his successor took any steps to review and revise the LFB’s operational policies, procedures and training to make sure that firefighters (and incident commanders in particular) understood how best to respond to a fire that had taken hold in the external wall of a high-rise building. Nor did they take any effective steps to ensure that control room staff received essential training.
The managerial weaknesses we have identified resulted in part from the historic separation between the departments responsible for operational matters and those responsible for support functions and a lack of effective communication between them. Historically, the Fire Safety department, like the control room, had become isolated from the operational departments, leading to a failure to communicate information about the dangers of combustible materials and a corresponding failure to ensure that they were taken into account in the policies and training. For a long time that failure was compounded by an entrenched but unfounded assumption that the regulatory regime in the Building Regulations was sufficient to prevent such dangers from arising in this country. After the Lakanal House fire senior officers recognised that compliance with the regulations could not be guaranteed, but no one appears to have thought that firefighters needed to be trained to recognise and deal with the consequences. That was partly because senior officers were confident that existing training and operational practices were comprehensive and that the additional measures identified following the Lakanal House fire had been implemented. The Grenfell Tower fire showed, however, the extent to which that confidence was misplaced.
Confidence in existing practices and procedures manifested itself in other ways. When a problem arose which called for careful and detailed consideration, on too many occasions the LFB’s response was that change was unnecessary or too difficult, even in matters which touched upon operational or public safety. The problems with radio communications in high-rise concrete buildings provide one example. Although they were well known and regularly encountered, no effective steps were taken to investigate them to identify reliable and effective solutions. The problems were simply considered too intractable. That attitude to perennial communications difficulties was unsustainable, primarily because they were a recurring feature of inquests into the deaths of both firefighters (as at the Shirley Towers fire) and members of the public (pre-eminently, at the Lakanal House fire). Given the evident danger to the life and safety of its personnel and the public, there were compelling reasons for the LFB to invest considerable effort in seeking to resolve the problems that had afflicted radio communications for so long, but regrettably nothing effective was done.
There is one further point that we need to address in this context. Although we acknowledge the strength of opinion held by some that the approach to funding public services adopted by the government between 2010 and 2015 and by the Mayor of London between 2012 and 2016 constrained the LFB’s operational effectiveness, none of the witnesses from whom we heard told us that insufficient financial or other resources had caused or contributed to the failings that occurred on the night of the Grenfell Tower fire. In that respect, it is telling that the LFB did not suggest that budgetary constraints had been responsible for any of its shortcomings and it is worth noting that the report of Her Majesty’s Inspectorate of Constabulary and Fire and Rescue Services on the LFB, published after the Phase 1 report on 17 December 2019, stated that, although the brigade was inefficient in its spending, it was not under-funded.[1772]
The tragic conclusion is that the Lakanal House fire in July 2009 forewarned the LFB about the existence of the shortcomings which revealed themselves once more on the night of 14 June 2017. Those shortcomings could have been avoided if the LFB had been more effectively led in a number of respects, particularly in its response to the Lakanal House fire, and if use had been made of its knowledge of the dangers flowing from modern materials and methods of construction. On any view, that is a serious indictment of an organisation whose principal purpose is to protect the public and of the quality of its leadership.
1) Phase 1 Report Volume IV, paragraph 31.14.
2) Hancox, Gas Engineering Report {RHX00000012/15} paragraphs 30-31 and figure 6.
3) Hancox, Gas Engineering Report {RHX00000012/13-14} paragraph 29 and figure 4.
4) Hancox, Gas Engineering Report {RHX00000012/23} paragraph 44.
5) Mason {CAD00003005/2} page 2, paragraphs 7-8.
6) Harrison {Day159/16:4-14}.
7) Harrison {Day159/17:4-8}; https://www.hse.gov.uk/regulating-major-hazards/energy-division.htm.
8) Harrison {Day159/18:7-16}.
9) Gas Act 1986 {INQ00014770/52-53} section 10; Mason {CAD00000004/2} page 2, paragraph 5.
10) Gas Act 1986 {INQ00014770/53} section 10(9)(b); Harrison {Day159/19:16}-{Day159/20:8}.
11) Pipelines Safety Regulations 1996 {INQ00014790/7} regulation 13; Pipelines Safety Regulations 1996 {INQ00014790/3} regulation 3(1)-(2).
12) Harrison {Day159/21:12-21}.
13) {CAD00000031}.
14) {CAD00000031} sheet 3: Riser Information, row 12, column AE; {CAD00000031} sheet 4: Lateral Information, row 9, column U; Hancox, Gas Engineering Report {RHX00000012/135} paragraph 310.
15) {CAD00000031} sheet 2: Supply Pipe Information, rows 11-12, column L; Hancox, Gas Engineering Report, {RHX00000012/68} paragraph 158.
16) {CAD00000031} sheet 4: Lateral Information, rows 7-12, column O; Hancox, Gas Engineering Report {RHX00000012/114-115} paragraph 248 and figures 65-66.
17) {CAD00000031} sheet 4: Lateral Information, row 9, column W; Hancox, Gas Engineering Report {RHX00000012/23-24} paragraph 44 and figure 17.
18) Harrison {CAD00002985/8} page 8, paragraphs 30-32.
19) {CAD00002984}.
20) Harrison {Day159/40:11-16}.
21) {RHX00000005/64} paragraph 7.3.1; Pipelines Safety Regulations 1996 {INQ00014790/7} regulation 13.
22) Pipelines Safety Regulations 1996 {INQ00014790/7} regulation 12; see also the duty to maintain the pipeline (including all its related apparatus) in an efficient state, efficient working order and in good repair: Pipelines Safety Regulations 1996 {INQ00014790/7} regulation 13.
23) Hancox, Gas Engineering Report {RHX00000012/220} paragraph 470; Harrison {CAD00002985/22} page 22, paragraph 82; Harrison {Day159/108:18}-{Day159/109:1}.
24) {CAD00002989/5}.
25) Hancox {Day161/41:10-20}.
26) Harrison {Day159/127:19-20}.
27) Phase 1 Report Volume IV, paragraph 31.4.
28) {CAD00002984/1}.
29) Harrison {CAD00002985/10-11} pages 10-11, paragraphs 37-39.
30) Harrison {CAD00002985/11} page 11, paragraph 41; Harrison {Day159/137:22}-{Day159/138:7}.
31) Harrison {Day159/137:22}-{Day159/138:7}; {Day159/138:22}-{Day159/139:5}; {Day159/140:8-14}; {CAD00002987/14} paragraph 5.6.3; {CAD00003001/13-15} paragraphs 6 and 9.
32) Harrison {CAD00003043/13-14} pages 13-14, paragraph 43; Cadent Module 3 submissions {CAD00003047/23} paragraphs 64-65.
33) Hancox, Gas Engineering Report {RHX00000012/110-111} figures 60-61 and paragraph 242.
34) {CAD00002174}; {CAD00002241}.
35) {CAD00000031} Supporting Photos sheet: row 3, column B.
36) Cadent Module 3 submissions {CAD00003047/18-19} paragraphs 50-52; Harrison {MET00018804/8} page 8, paragraph 31.
37) Cadent employee Jason Allday and surveyor Simon Boygle.
38) {MET00018309/2-4}; Phase 1 Report Volume IV, paragraph 31.3.
39) Hancox {Day161/58:22}-{Day161/59:3}.
40) {CAD00002957}; Hancox, Gas Engineering Report {RHX00000012/74} paragraph 174 and figure 41; Harrison {Day159/145:5-14}.
41) Hancox {Day161/8:23}-{Day161/9:1}; Harrison {Day159/33:8-23}; Dolan {Day160/17:20}-{Day160/18:11}.
42) Dolan {Day160/17:2-18}.
43) Hancox {Day161/20:24}-{Day161/21:16}.
44) {RHX00000005}.
45) Dolan {MET00012711/2} page 2, paragraphs 7-10.
46) Dolan {MET00012711/4-7} pages 4-7, paragraphs 23-28.
47) Dolan {Day160/29:21}-{Day160/30:2}.
48) {CAD00000059}; Mason {CAD00003005/8} page 8, paragraph 23.
49) Gas Act 1986 {INQ00014770/53} section 10(9).
50) {RHX00000005/29-31} paragraph 4.2.1.4.
51) Dolan {MET00012711/8-9} pages 8-9, paragraph 34; Dolan {Day160/53:4-10}.
52) Dolan {MET00012711/8} page 8, paragraph 31; Dolan {Day160/62:11-23}; Hancox {Day161/112:7}-{Day161/113:7}.
53) Dolan {MET00012711/9} page 9, paragraph 35; Mason {CAD00003005/11} page 11, paragraph 39; Dolan {Day160/64:20}-{Day160/65:12}.
54) Hancox {Day161/113:9-25}.
55) {RHX00000005/52} paragraph 6.4.3.1.
56) {RHX00000005/52} paragraph 6.4.3.5.
57) {RHX00000005/52} paragraph 6.4.3.2; {CAD00000054/2-3}; Dolan Day160/66:21}-{Day160/67:8}.
58) {RHX00000005/54-55} figures 18-19.
59) {CLG00000224/81} paragraph 8.41.
60) {CLG00000224/81} paragraph 8.41.
61) {CAD00000054}; updated on 1 November 2016 {CAD00000038}.
62) Dolan {Day160/55:24}-{Day160/56:14}.
63) {RHX00000005/52} paragraph 6.4.3.3; {CLG00000224/32} paragraph 2.42.
64) {CLG00000224/32} paragraph 2.35.
65) {CLG00000224/116} diagram 52.
66) Fire Precautions in the design, construction and use of buildings – Part 5: Access and facilities for firefighting {BSI00000087/23} paragraph 7.1.4. While BS 5588-5 was superseded by BS9999:2008 (and ADB therefore referred to an out of date standard), identical provisions appeared in BS9999:2008 at paragraph 27.2.7.2, to the effect that only services associated with firefighting should pass through the firefighting shaft {BSI00000064/123}.
67) {CLG00000224/81} Note to paragraph 8.40. Neither BS 5580-5:2004 nor BS9999:2008 make any such provision.
68) Dolan {Day160/91:19}-{1Day160/92:14}; Hancox {Day161/117:7-18}.
69) {TMO10015305}; {TMO10016548}; {CST00001240}.
70) {TRI000000263}.
71) {RHX00000005/52} paragraph 6.4.3.5.
72) Dolan {Day160/101:6-10}; {Day160/104:4-9}.
73) Hancox, Gas Engineering Report {RHX00000012/30} figure 22; Thompson {TRI00002923/2} page 2, paragraph 8; Images of louvred doors {TRI00002921}; {TRI00002922}; Dolan {Day160/105:3-15}.
74) Hancox, Gas Engineering Second Supplementary Report {RHX00000027/21} paragraph 44.
75) Hancox, Gas Engineering Second Supplementary Report {RHX00000027/22} paragraph 50; Dolan {Day160/105:15-23}; Hancox {Day161/135:5-18}.
76) {TRI000000392}.
77) Dolan {Day160/102:3}-{Day160/103:9}; {Day160/103:16-22}; {Day160/148:2-14}.
78) Hancox, Gas Engineering Report {RHX00000012/191} paragraph 385; Hancox, Gas Engineering Report {RHX00000012/195} paragraph 394; Hancox {Day161/139:15-17}.
79) Hancox {Day161/142:8-11}.
80) {RHX00000005/28} paragraph 4.2.1.1; {RHX00000005/94-102} Appendix 3.
81) {TRI000000369}.
82) {TRI000000369}.
83) Dolan {Day160/85:14-16}.
84) Hancox {Day161/150:10}-{Day161/151:9}; {Day161/172:3-16}.
85) {TRI000000369} at “MOBS” where a red “high-risk” categorisation is shown in the final column.
86) Dolan {Day160/89:11-23}.
87) The Construction (Design and Management) Regulations 2015 {INQ00011316/7} regulation 6; The Construction (Design and Management) Regulations 2015 {INQ00011316/29} regulation 6, schedule 1.
88) {TRI000001784}.
89) Lane, Phase 2 Report Version 2 {BLARP20000016/148-149} paragraphs 11.3.1-11.3.9.
90) Harrison {Day159/84:5-14}; Dolan {CAD00003044/13} page 13, paragraphs 51-52.
91) Hancox, Gas Engineering Report {RHX00000012/14} paragraph 29 (c) and figure 4.
92) Hancox, Gas Engineering Report {RHX00000012/31} figure 24.
93) {CAD00001643}; {CAD00001640}.
94) {TRI000000263}; {TRI000001431}.
95) Hancox, Gas Engineering Report {RHX00000012/26} figure 18.
96) Dolan {Day160/125:7-9}.
97) Dolan {Day160/125:7}-{Day160/126:10}.
98) Dolan {MET00012711/11} page 11, paragraph 47.
99) Dolan {Day160/140:16}-{Day160/141:10}.
100) Dolan {Day160/139:23}-{Day160/140:10}.
101) Dolan {Day160/141:20}-{Day160/142:8}.
102) Dolan {Day160/144:13-25}; {Day160/145:15}-{Day160/146:3}; {TRI000001223}.
103) {TRI000001223}.
104) Dolan {Day160/157:16-23}; Hancox, Gas Engineering Report {RHX00000012/194} paragraph 391.
105) Hancox, Gas Engineering Report {RHX00000012/195-196} paragraphs 395-396; Hancox {Day161/158:3-16}.
106) Hancox {Day161/161:3-13}.
107) Hancox {Day161/154:15}-{Day161/155:4}.
108) {TRI000001218}.
109) {TRI000001218/4}.
110) Hancox, Gas Engineering Report {RHX00000012/156} paragraph 354; Dolan {Day160/171:1-15}; Hancox {Day161/173:3-9}.
111) Dolan {Day160/162:10-19}; {Day160/170:15-25}.
112) Dolan {Day160/186:9}-{Day160/187:9}; Hancox {Day161/156:14-25}.
113) Dolan {Day160/189:21-25}.
114) {TRI000001218}.
115) {TMO10016548}.
116) {TRI000001377}; Dolan {Day160/189:14-25}; Hancox, Gas Engineering Report {RHX00000012/196} paragraph 397.
117) Dolan {Day160/72:24}-{Day160/73:10}.
118) Hancox, Gas Engineering Report {RHX00000012/33} paragraph 61.
119) {RHX00000005/38} paragraph 5.2.3.
120) Hancox, Gas Engineering Report {RHX00000012/58-61} paragraph 133(f).
121) Hancox, Gas Engineering Report {RHX00000012/161} paragraph 364.
122) Dolan {Day160/190:18}-{Day160/191:1}.
123) {MET00016651}.
124) {MET00016558}; Hancox, Gas Engineering Report {RHX00000012/159} paragraph 362.
125) Hancox, Gas Engineering Report {RHX00000012/117} paragraph 252.
126) Dolan {TRI00001797/2-3} pages 2-3 paragraph 7; Mason {CAD00003005/11} page 11, paragraph 34.
127) {MET00016722}; {MET00016516}.
128) {MET00016516} showing smoke staining at the top of the boxed portion of gas riser on floor 17; {MET00016533} showing staining at the bottom of boxed portion of gas riser on floor 16; Hancox, Gas Engineering Report {RHX00000012/178-179}.
129) {TRI000000985/3}.
130) Hancox {Day161/166:8}-{Day161/170:6}.
131) Dolan {Day160/175:15}-{Day160/176:20}.
132) Hancox, Gas Engineering Report {RHX00000012/187} paragraph 375.
133) Stokes {CST00003063/47} page 47, paragraph 138; {TRI000000405}.
134) Dolan {Day160/110:20}-{Day160/111:8}.
135) {TMO10016428/1}.
136) {TMO10016546}.
137) {TRI000000405}; Dolan {Day160/111:1-8}.
138) Dobson {LFB00032157/2} page 2, paragraph 5.
139) Dobson {LFB00032737/2-3} pages 2-3, paragraph 5.
140) Phase 1 hearing: {Day50/10:3-12}.
141) Section 1(2)(c) of the Fire and Rescue Services Act 2004, which came into force with effect from 1 April 2018 under The Policing and Crime Act 2017, section 9 and The Policing and Crime Act 2017 (Commencement No. 7) Regulations 2018, regulation 4
142) Dexter {LFB00032363/2} page 2, paragraph 4.
143) Dexter {LFB00032363/2} page 2, paragraph 5.
144) Also later known as ‘Operations and Mobilising’.
145) Brown {LFB00032166/3} page 3, paragraph 7.
146) Brown {Day186/7:17}-{Day186/8:1}; Brown {Day186/5:2-21}.
147) Brown {LFB00032166/23} page 23, paragraph 74.
148) Daly {Day183/13:24}-{Day183/16:19}.
149) Jack {LFB00032244/3} page 3, paragraph 7.
150) Daly {LFB00032306/3} page 3, paragraph 9.
151) Daly {Day183/29:12-22}; Daly {Day183/39:4-21}.
152) Daly {Day183/18:1-20}.
153) Daly {MET00077774/16}.
154) Daly {Day183/51:8-21}.
155) Cohen-Hatton {Day185/59:18}-{Day185/61:14}.
156) Daly {MET00077774/16-17}; Daly {Day183/58:23-25}.
157) Daly {Day183/61:24}-{Day183/62:5}.
158) Daly {Day183/32:7-10}.
159) Daly {Day183/29:12-22}.
160) Daly {Day183/35:1-8}.
161) Daly {Day183/38:2-15}.
162) Daly {Day183/28:2-22}.
163) Daly {Day183/14:7-18}.
164) Dexter {Day178/30:1-24}.
165) Reason {LFB00032747/2} page 2, paragraph 7.
166) Reason {Day180/93:3-7}; Cowup {LFB00032784/3} page 3, paragraph 10.
167) Cotton {Day208/10:8-11}.
168) Cotton {Day208/10:12}-{Day208/11:3}; Cotton {Day208/8:3-13}.
169) Cotton {Day208/30:16}-{Day208/32:1}; {Day208/33:24}-{Day208/34:4}; {LFB00067840} is an example of the reports produced by the department.
170) Cotton {Day208/12:21}-{Day208/13:10}.
171) Cotton {Day208/31:2-12}.
172) Cohen-Hatton {LFB00110660/2} page 2, paragraph 10.
173) Reason {Day180/93:8-15}.
174) Brown {Day186/10:7-21}.
175) {LFB00000010}.
176) Brown {LFB00032166/4} page 4, paragraph 9; George {LFB00032823/2} page 2, paragraph 6.
177) Groves {Day177/11:4-13}.
178) Apter {LFB00067794/2} page 2, paragraph 4.
179) Dobson {Day210/59:20-25}; {Day210/63:4-25}.
180) Dobson {Day210/62:1-10}; {Day210/64:25}-{Day210/65:6}.
181) Dobson {Day210/64:21}-{Day210/65:11}.
182) {LFB00040625/2}; Dexter {Day178/53:19}-{Day178/55:6}.
183) Operational Resilience and Training and the Deputy Commissioner’s directorate before the 2015 restructuring; Operations and Safety and Assurance following the restructuring.
184) Cotton {Day208/27:10-18}.
185) Brown {LFB00084020/19} page 19, paragraph 50; {LFB00040652/1} paragraph 2.
186) Phase 1 Report Volume IV, pages 589-590, paragraphs 27.16-27.20.
187) {LFB00012695/2} page 2, paragraph 1.5.
188) Dexter {Day178/69:21}-{Day178/70:3}.
189) {LFB00055171/2} page 2, paragraphs 1.2 and 1.5; Dexter {Day178/75:17}-{Day178/76:3}.
190) {LFB00055171/8} page 8, paragraph 3.41.
191) Dexter {Day178/69:1-5}.
192) {LFB00055171/4} page 4, paragraphs 3.1-3.2.
193) Cohen-Hatton{LFB00110660/16} page 16, paragraph 58.
194) Dexter {Day178/78:5}-{Day178/79:12}.
195) {LFB00055171/4} page 4, paragraph 3.3.
196) Dexter {Day178/105:25}-{Day178/106:3}. “IMPD report” refers to the six-monthly reports presented to the co-ordination board. “IMP report” refers to the individual reports produced following meetings to review operational responses and incident command. which provided material for the database.
197) Dexter {Day178/82:20-24}; Cotton {Day208/38:9-12}.
198) {LFB00067840/5-6}.
199) Cotton {Day208/40:12}-{Day208/41:16}; Cohen-Hatton {Day184/205:14-22}.
200) Cotton {Day208/40:21}-{Day208/41:6}.
201) Dexter {Day178/82:20}-{Day178/83:7}.
202) Cotton {Day208/41:17}-{Day208/43:23}.
203) Dexter {Day178/91:8-25}.
204) Dexter {Day178/83:8-25}; Cotton {Day208/44:2}-{Day208/45:10}.
205) Spooner {MET00078859/4} page 4, paragraph 4.
206) {LFB00120998}.
207) Dexter {Day178/165:6}-{Day178/166:6}.
208) Groves {Day177/29:3-4}; Dexter {Day178/72:10-15}.
209) Cotton {Day208/55:2-11}.
210) Dexter {Day178/111:9-16}; Cotton {Day208/61:17}-{Day208/62:9}.
211) {LFB00036796/4} for example, in relation to Fire Survival Guidance policy.
212) Cotton {Day208/72:3}-{Day208/73:2}.
213) {LFB00032798/2} page 2.
214) Cotton {Day208/73:21}-{Day208/75:7}.
215) Cotton {Day208/77:25}-{Day208/79:5}; Groves {Day177/100:18-22}.
216) Groves {Day177/88:25}-{Day177/89:15}.
217) Groves {Day177/94:22}-{Day177/95:5}.
218) Groves {Day177/84:11}-{Day177/85:12}.
219) Groves {Day177/94:17}-{Day177/96:15}.
220) Cotton {Day208/80:25}-{Day208/81:3}.
221) Cotton {Day208/82:4-16}.
222) Dexter {Day178/149:25}-{Day178/151:15}
223) Dexter {Day178/157:6}-{Day178/158:19}.
224) Dexter {Day178/152:3-13}.
225) {LFB00067818/2}.
226) {LFB00123806}.
227) {LFB00040719/2}; Cotton {Day208/88:10}-{Day208/90:9}.
228) Reason {Day180/100:12}-{Day180/103:22}.
229) Groves {Day177/12:14-20}; {Day177/52:6-11}.
230) Groves {Day177/14:7}-{Day177/15:3}.
231) Groves {Day177/8:16}-{Day177/9:7}.
232) Groves {Day177/8:3-13}.
233) Groves {Day177/20:12}-{Day177/21:4}.
234) Groves {Day177/21:8-19}.
235) Groves {Day177/22:20}-{Day177/23:22}.
236) Groves {Day177/35:8-23}; Groves {MET00071103/11}.
237) Groves {LFB00102138/29} page 29, paragraph 49.
238) Groves {Day177/45:3-14}.
239) Groves {LFB00102138/22} page 22, paragraph 32.
240) Groves {LFB00102138/23} page 23, paragraph 33; Groves {Day177/65:25}-{Day177/66:11}.
241) Groves {Day177/65:12-24}; {Day177/67:18-25}.
242) Graham Ellis {LFB00118230/15} page 15, paragraph 69; Reason {Day181/30:16-23}.
243) Groves {Day177/47:16}-{Day177/48:9}; {Day177/48:20-25}.
244) Groves {Day177/55:2-19}.
245) Groves {Day177/52:6-11}.
246) {LFB00067786/33}.
247) Groves {Day177/56:17}-{Day177/57:5}; Reason {Day180/106:10-22}; Cotton {Day208/65:7-8} and Dexter {Day178/125:6-8}.
248) {LFB00055127/23} page 23, paragraph 7.1; Groves {Day177/68:15}-{Day177/69:23}.
249) Groves {Day177/70:2}-{Day177/71:8}.
250) {LFB00055171/13} page 13, paragraph 6.10.
251) Groves {Day177/71:21}-{Day177/73:7}.
252) Groves {Day177/74:16-25}.
253) Groves {Day 177/82:8-12}.
254) McGuirk, Firefighting Expert Report {SMC00000046/47-50} pages 47-50, paragraphs 123-126.
255) Phase 1 Report Volume IV paragraph 27.16.
256) {LFB00032158/2-3}.
257) Reason {Day180/169:1}-{Day180/170:8}; Cotton {Day208/157:10}-{Day208/159:10}; {Day208/160:5}-{Day208/162:7}.
258) {LFB00034062/22}.
259) {LFB00067820/13-14}, action 3; {LFB00003716/5}; {LFB00038170}; Reason {Day181/28:7}-{Day181/55:13}.
260) {LFB00038170}.
261) Reason {Day181/49:2}-{Day181/50:21}; {Day181/54:14-23}.
262) {LFB00038170}; {LFB00115289}.
263) {LFB00067820/13-14}.
264) {LFB00038170}; {LFB00115289}.
265) {LFB00067832/24-25}.
266) Reason {Day181/84:3-18}.
267) Reason {LFB00067846/13-14} pages 13-14, paragraph 17; Reason {Day181/48:12}-{Day181/50:21}; {Day181/82:11}-{Day181/84:18}.
268) Reason {Day180/150:11}-{Day180/151:8}; {Day180/157:1-7}.
269) Cotton {Day208/224:21}-{Day208/226:12}; {Day208/235:7-25}.
270) Cotton {Day209/17:17}-{Day209/21:21}.
271) Hayward {Day201/30:1-10}.
272) {LFB00094806/2}; {LFB00118750}; Reason {Day181/101:11}-{Day181/109:18}; {Day181/141:14}-{Day181/148:5}.
273) {LFB00003716}; Reason {Day181/62:16}-{Day181/75:20}; Cotton {Day209/2:10}-{Day209/3:10}; {Day209/13:11-18}.
274) {BAB00000011}; Reason {Day181/110:10}-{Day181/129:21}.
275) Reason {Day181/128:18}-{Day181/129:21}.
276) {LFB00004801/29}, action 3b; Groves {Day177/123:12}-{Day177/127:13}.
277) {LFB00003716}; {LFB00115289}; Reason {Day181/73:4-22}.
278) Reason {Day181/76:2}-{Day181/77:12}.
279) {LFB00067812/5}.
280) {LFB00042089}; {LFB00067832/25}; {LFB00003716/8}.
281) {LFB00042089}; {LFB00073973}.
282) {LFB00043552}; Reason {Day181/130:1}-{Day181/138:10}; Cotton {Day209/40:6}-{Day209/47:23}.
283) Reason {Day180/100:12}-{Day180/103:22}.
284) {LFB00042089}.
285) Cotton {Day208/208:3}-{Day208/210:17}; Cohen-Hatton {Day185/69:9-14}.
286) Groves {Day177/140:16}-{Day177/141:18}; Cotton {Day209/73:21}-{Day209/76:23}.
287) Groves {Day177/142:11}-{Day177/143:7}; Cotton {Day209/75:22}-{Day209/76:4}.
288) Cotton {Day209/76:5}-{Day209/77:15}.
289) Ellis {LFB00118230/15} page 15, paragraphs 69-71; Groves {Day177/46:3}-{Day177/55:19}; {Day177/116:7}-{Day177/120:24}; Reason {Day181/30:16-23}; {Day181/70:5}-{Day181/73:3}; Cotton {Day208/205:21}-{Day208/206:3}; {Day208/206:19}-{Day208/207:3}; {Day209/15:23}-{Day209/17:7}; {Day209/26:4-13}; {Day209/76:5}-{Day209/78:11}; {LFB00118213/11}; Dobson {Day211/186:24}-{Day211/188:21}; {Day211/190:6}-{Day211/192:9}.
290) Cotton {Day209/76:5}-{Day209/79:12}.
291) Dobson {Day211/127:19}-{Day211/128:14}.
292) Dobson {Day211/185:23}-{Day211/192:9}.
293) Dobson {Day211/178:12-23}.
294) Reason {Day181/36:5-17}.
295) Reason {Day181/137:1-13}.
296) {LFB00118186}.
297) The FRSs consulted were Tyne and Wear, Greater Manchester, Hampshire, Derbyshire and Hertfordshire.
298) Cohen-Hatton {Day185/125:4-15}.
299) Cohen-Hatton {Day185/145:11-16}; {Day185/147:1-15}.
300) {LFB00118193}.
301) {LFB00118189}.
302) Cohen-Hatton {LFB00110660/24} page 24, paragraph 87; {LFB00118192/2}.
303) {LFB00118187}; Cohen-Hatton {Day185/163:1-17}.
304) Cohen-Hatton {Day185/164:4-8}.
305) {INQ00014796/39}.
306) Phase 1 Report Volume IV paragraph 27.9.
307) Phase 1 Report Volume IV paragraph 27.10.
308) {LFB00031816/5-6}.
309) {LFB00031816/6}.
310) {CLG00019478}.
311) {CLG00019478/8} paragraph 10.
312) {CLG00019478/9-10} paragraphs 18-20.
313) Dexter {Day179/94:9-18}.
314) Dobson {Day210/102:19}-{Day210/103:12}.
315) Dexter {Day179/94:19-23}; Dobson {Day210/103:9-20}.
316) Dobson {Day210/103:21}-{Day210/104:16}.
317) {LFB00001805}.
318) {LFB00001805/1}.
319) Dobson {Day210/117:9-16}.
320) Dobson {Day210/73:6-10}.
321) Dobson {Day210/75:8-20}.
322) The LFB’s Lakanal Control Report, produced for the purpose of the Lakanal inquests, identified five calls to the control room during which fire survival guidance advice was given {HOM00001124/35-37}. Two of those calls were from the same flat and three of the calls were in progress at the same time.
323) Dobson {Day210/75:21}-{Day210/76:13}.
324) {LFB00039696} Lakanal House Board Terms of Reference; Dobson {Day210/79:3}-{Day210/80:15}.
325) Dobson {Day210/86:21}-{Day210/87:3}.
326) {LFB00084031/7-10}.
327) {LFB00084032/5-8}.
328) Dobson {LFB00032157/10} page 10, paragraph 38; Reason {LFB00032747/18} page 18, paragraph 53; Dobson {Day211/153:12-24}.
329) Lindridge {LFB00083925/4} page 4, paragraph 17.
330) Cotton {LFB00032737/6} page 6, paragraph 21.
331) Lindridge {LFB00083925/3} page 3, paragraph 12.
332) {LFB00033943}.
333) {LFB00033943/4-5} pages 4-5, paragraphs 5.2 and 5.3.
334) {LFB00083988}.
335) {LFB00083988/6-23}.
336) Cotton {Day208/110:10}-{Day208/111:6}.
337) Dobson {Day211/171:3}-{Day211/172:7}.
338) Reason {Day180/130:19-25}; Dobson {Day211/172:8-25}.
339) Dobson {Day210/88:15}-{Day210/89:5}; {Day211/171:24}-{Day211/172:4}.
340) Reason {Day180/130:15-18}.
341) Reason {LFB00032747/19} page 19, paragraph 58; Reason {Day180/132:4}-{Day180/133:6}.
342) Cotton {Day208/114:5-19}.
343) Cotton {Day208/139:1-22}.
344) {LFB00032158}.
345) Reason {LFB00032747/5} page 5, paragraph 19.
346) Reason {Day180/139:2}-{Day180/140:21}.
347) {LFB00073406}; {LFB00034062}.
348) Reason {Day180/141:5}-{Day180/142:16}.
349) Reason {Day180/142:9}-{Day180/143:7}.
350) {LFB00042089}.
351) Reason {LFB00032747/6} page 6, paragraph 22.
352) Reason{Day180/145:6}-{Day180/146:8}.
353) Cotton {LFB00032737/7} page 7, paragraph 25.
354) {LFB00089127}.
355) Dobson {LFB00032157/7} page 7; Dobson {Day210/100:14}-{Day210/101:3}.
356) {LFB00032156/3}.
357) Dobson {LFB00032157/7} page 7, paragraph 23; {LFB00032156/3}.
358) Reason {Day180/148:18-23}; Dobson {Day210/96:7-18}.
359) Reason {Day180/131:6}-{Day180/132:3}; {Day180/133:7-22}.
360) Reason {LFB00032747/7-8} pages 7-8, paragraphs 27 and 30.
361) Reason {Day180/151:4-8}.
362) {LFB00089117}.
363) {LFB00029746}.
364) {LFB00032156/3}.
365) {LFB00067819/1}, {LFB00067819/5}.
366) Reason {Day181/143:6}-{Day181/144:11}.
367) Reason {Day181/144:12-18}.
368) Reason {Day181/147:15-25}.
369) Reason {Day181/144:3}-{Day181/146:13}.
370) {LFB00123737/11} page 11, paragraph 26.
371) Dobson {Day210/131:18}-{Day210/132:9}; {Day210/132:16}-{Day210/133:5}.
372) Crowder {Day230/4:15-21}.
373) Sir Ken Knight {Day245/187:11-13}.
374) This was clear from firefighters’ evidence at the inquests following the Lakanal House fire: https://www.lambeth.gov.uk/about-council/transparency-open-data/lakanal-house-coroner-inquest.
375) {HOM00002128/12}.
376) Johnson, Expert Communications Report {CWJ00000010/83} page 83.
377) Johnson, Expert Communications Report {CWJ00000010/35} page 35.
378) {HOM00045826/34-35} page 34-35.
379) {LFB00001232}.
380) Dobson {Day210/119:17}-{Day210/120:1}.
381) Dobson {Day210/120:11-21}.
382) {LFB00004801/16} page 16, action 20; {LFB00033943/15} page 15, action 20.
383) Dexter {Day179/82:21-25}.
384) {LFB00004801/16} page 16, action 20, {LFB00051803/135}; see also {LFB00033943/15} page 15, action 20.
385) {LFB00096647}.
386) Dexter {Day179/86:12-23}.
387) {LFB00083970}.
388) {LFB00025654/13-14}.
389) {LFB00025654/3} page 3.
390) {LFB00025654/3} page 3, paragraph 18.
391) Dobson {Day210/135:13-24}.
392) Dobson {Day210/135:24}-{Day210/136:2}.
393) Dobson {Day210/136:4-9}.
394) Mr Dobson was referring to observations made by Mr Justice MacDuff, the judge who presided over the trial of the incident commanders at the Atherstone-on-Stour fire in November 2007 and was critical of the large volume of operational guidance notes and other materials considered during the trial, Dobson {Day210/140:4-25}; see also {LFB00046278/21}.
395) Dobson {Day210/141:1-22}.
396) {LFB00032154}, Brandon Lewis {Day257/3:4-7}.
397) Dobson {Day210/152:23}-{Day210/153:5}.
398) See Part 2, Chapter 9.
399) {LFB00032158}.
400) {CLG00000401/2}.
401) {HOM00047743}.
402) Daly {Day183/157:3-4}.
403) {LFB00004801/29} page 39, action 3c.
404) Reason {Day181/14:18-19}.
405) {BAB00000073}; {LFB00030044}.
406) {LFB00004801}.
407) {LFB00004801/13} page 13, action 6; {LFB00004801/15} page 15, action 14; {LFB00004801/17-18} pages 17-18, actions 21-23; Reason {Day180/177:9}-{Day180/178:6}, {Day180/208:10}-{Day180/209:8}, {Day181/37:16}-{Day181/38:17}, {Day181/88:18}-{Day181/89:13}; Daly {Day184/11:11-17}, {Day184/126:5-19}; David Brown {Day187/73:23}-{Day187/75:16}; Cowup {Day195/116:11-20}; Cotton {Day208/194:13-17}; Dobson {Day211/6:6-11}, {Day211/11:24}-{Day211/12:4}.
408) Reason {Day180/208:17}-{Day180/209:8}.
409) Reason {Day180/209:3-4}.
410) Reason {Day180/210:11-16}.
411) Reason {Day180/196:4}-{Day180/197:8}; {Day180/205:16)-{Day180/206:24}; {Day180/208:10)-{Day180/211:10}; {Day181/3:5}-{Day181/8:16}; Cotton {Day208/192:3}-{Day208/193:8}; {Day208/194:13}-{Day208/195:23}.
412) {LFB00123737/47} page 47, paragraph 131.
413) Roe {Day212/155:2-12}.
414) Reason {Day181/9:3-22}.
415) Reason {Day181/11:3-9}.
416) Reason {LFB00067846/28} page 28, paragraph 61; Reason {Day181/20:2}-{Day181/22:1}.
417) Reason {Day181/88:18}-{Day181/89:13}, {Day180/177:9}-{Day180/178:6}, {Day181/37:16}-{Day181/38:17}; David Brown {Day187/73:23}-{Day187/75:16}; Cowup {Day195/116:11-20}; Dobson {Day211/6:6-11}, {Day211/11:24}-{Day211/12:4}.
418) Reason {Day181/3:23}-{Day181/5 -18}.
419) Dobson {Day211/4:16}-{Day211/6:19}; {Day211/26:19}-{Day211/27:14}.
420) Cowup {Day195/49:1-8}, {Day195/163:5-7}, Dobson {Day211/11:16}-{Day211/12:8}, {Day211/44:15-23}, {Day211/6:6-11}, Cotton {Day208/178:5-19}.
421) {LFB00028515}.
422) Bureau Veritas report {LFB00028515/91-94}; LFB report {LFB00028515/95-102}.
423) {LFB00028515/64}.
424) {LFB00028515/117-122}.
425) Dobson {Day211/26:11-18}.
426) Dobson {Day211/26:19}-{Day211/27:14}.
427) Dexter {Day179/95:21}-{Day179/97:19}; Reason {Day182/101:2}-{Day182/102:25}; Daly {Day183/117:22}-{Day183/136:9}; {Day183/163:8}-{Day183/164:8}; Cotton {Day209/231:10}-{Day209/232:11}; Cotton {Day209/233:11-21}; Dobson {Day211/33:4}-{Day211/36:1}.
428) Daly {Day183/170:12}-{Day183/178:17}.
429) {LFB00024217}.
430) {INQ00014890}.
431) Cotton {Day210/9:12-13}.
432) {LFB00032916/2-4}.
433) {LFB00032916/5-9}.
434) Daly {Day183/135:12}-{Day183/136:9}; {Day183/145:16}-{Day183/146:13}.
435) {LFB00032892/10-11}.
436) {LFB00032891/14}.
437) {LFB00032895/6}.
438) {LFB00032922/21-22}.
439) {LFB00032916}. It was produced in draft in July 2016 and finalised in October 2016 after the fire at Shepherd Court.
440) Cotton {Day209/233:22}-{Day209/234:5}.
441) Cotton {Day210/3:18}-{Day210/4:17}; {Day210/19:4}-{Day210/28:17}.
442) Cotton {Day210/5:3}-{Day210/6:13}.
443) {LFB00001708}.
444) Contemporaneous documents referred variously to 9 and 24 fire survival guidance calls: {LFB00001711}; {LFB00031757}.
445) {LFB00035092/5}; FSG database {LFB00031757}; Smith {Day202/201:1-20}.
446) {HOM00001124}.
447) {MET00080605/13}.
448) {LFB00001708/2}; {LFB00035109}.
449) Biles {MET00080605/7-8} pages 7-8.
450) {MET00080621}.
451) {LFB00118245}; {LFB00000084}.
452) {LFB00060951/8}.
453) Hanks {LFB00032724/2} page 2, paragraph 5.
454) Hanks {LFB00032724/2-3} pages 2-3, paragraph 6.
455) Hanks {LFB00032724/3} page 3, paragraph 7.
456) Hanks {LFB00032724/4-5} pages 4-5, paragraph 8.
457) {LFB00000084/8} paragraph 4.26.
458) Roe {LFB00060655/9} page 9, paragraph 21; Roe {LFB00083834/7-8} pages 7-8, paragraph 28; Closing statement for Modules 5 and 6 {LFB00123737/14} paragraph 35; {LFB00123737/35} paragraph 93.
459) Phase 1 Report Volume IV {INQ00014817/87} paragraph 27.3.
460) McGuirk Report {SMC00000046/35} paragraph 83.
461) Cowup {Day195/63:20}-{Day195/67:21}.
462) Dobson {Day211/127:10-12}.
463) Cowup {Day195/66:1-22}.
464) {MET00080621}; {LFB00120998}.
465) Roe {Day213/147:15-23}.
466) Roe {Day213/147:5-23}.
467) Phase 1 Report Volume IV {INQ00014817/108} paragraphs 28.53 and 28.54.
468) Daly {MET00077774/4}; Daly {Day183/206:11-18}.
469) Daly {Day183/205:17}-{Day183/206:13}.
470) Daly {Day183/210:24}-{Day183/211:20}.
471) {LFB00052135/6}.
472) {LFB00000091/2-4} paragraphs 3.5 and 3.6.
473) Green {LFB00032917/1-2} pages 1-2, paragraphs 3-5; Green {LFB00032917/5} page 5, paragraphs 23-26.
474) {LFB00032916/15-20}.
475) Daly {Day183/138:24}-{Day183/139:11}; {Day183/142:9}-{Day183/143:16}.
476) Closing statement in Modules 5 and 6 {LFB00123737/19} paragraphs 44 and 45.
477) {LFB00025654}; Daly {Day184/85:3-5}.
478) {LFB00025654/1}.
479) {LFB00025654/2} paragraph 1.
480) Daly {Day184/88:2-14}.
481) {LFB00025654/3-4}.
482) {LFB00025654/10}.
483) {LFB00025654/11-12}.
484) {LFB00025654/12} paragraphs 11 and 13.
485) Daly {Day184/92:12-13}.
486) Daly {Day184/94:9-13}.
487) Daly {Day184/94:22}-{Day184/95:20}.
488) {LFB00000155/6} paragraph 37.
489) Daly {Day184/112:13-24}.
490) Jack {LFB00120308/18} page 18, paragraph 61; {LFB00120296}.
491) {LFB00032153}.
492) {LFB00120301}; Daly {Day184/65:14-22}. The report refers to the “Performance Management Board”, which Dan Daly clarified in his evidence was likely to be a typographical error: {Day184/67:2-15}.
493) {LFB00120301/2}.
494) {LFB00120301/3}.
495) {LFB00120301/3}; {LFB00120301/8}.
496) Daly {Day184/74:1}-{Day184/75:1}.
497) Daly {Day184/78:19-24}.
498) Daly {Day184/76:10}-{Day184/77:4}.
499) {CLG10009016}.
500) Cotton {Day210/28:5-17}.
501) Cotton {Day210/26:21}-{Day210/27:15}.
502) Phase 1 Report Volume IV, paragraph 27.30
503) Phase 1 Report Volume IV, paragraphs 27.36.
504) Phase 1 Report Volume IV, paragraphs 27.22, 27.24 and 27.37.
505) Phase 1 Report Volume IV, paragraphs 27.35 and 27.37.
506) McGuirk {Day190/11:18-23}; {Day190/12:2-11}; {Day190/13:12-23}; {Day190/15:7-24}.
507) McGuirk {Day190/14:9}-{Day190/15:2}.
508) {HOM00045364}.
509) McGuirk {Day190/16:7-16}.
510) McGuirk {Day190/18:5}-{Day190/19:14}; {Day190/37:7-25}.
511) McGuirk {Day190/20:1-8}.
512) {HOM00045364/85}.
513) McGuirk {Day190/25:25}-{Day190/26:23}.
514) McGuirk, Firefighting Report {SMC00000046/15} paragraph 21.
515) {LFB00083849}; {LFB00001256}.
516) {LFB00003596}.
517) Phase 1 Report Volume IV, paragraph 27.30.
518) {LFB00083849/4}; {LFB00083849/7} paragraph 7.20.
519) {LFB00012734}.
520) {LFB00122962}.
521) North Kensington, Kensington and Chelsea fire stations.
522) {LFB00025654}.
523) Daly {Day183/46:10}-{Day183/47:11}; {Day184/107:17}-{Day184/108:7}.
524) Dobson {Day211/210:14-19}; Roe {Day213/122:10-19}.
525) Brown {Day187/38:8-14}; {Day187/40:8-14}.
526) {LFB00001255/18}.
527) The full list is set out in the Phase 1 Report Volume IV, paragraph 27.23.
528) McGuirk, Firefighting Report {SMC00000046/33-34} paragraphs 79 and 80.
529) Brown {Day211/197:22}-{Day211/198:8}.
530) Brown {Day186/54:15-20}. PN800 required all premises that scored 150 or above on the risk assessment to be recorded on the ORD {LFB00083849}.
531) Brown {Day186/55:4-22}; {Day186/101:5-15}.
532) {LFB00004801/28}.
533) Roe {Day213/125:8-20}.
534) {LFB00032161}.
535) Brown {Day186/59:16-25}.
536) {LFB00082695}.
537) {LFB00047224}.
538) Brown {Day186/69:19}-{Day186/70:1}.
539) Brown {Day186/7:17}-{Day186/18:1}.
540) Brown {Day186/29:17}-{Day186/32:4}.
541) Brown {Day186/32:15}-{Day186/33:7}.
542) Brown {Day186/37:13}-{Day186/38:3}.
543) Dobson {Day211/208:15-24}.
544) Brown {Day186/40:11-21}.
545) Brown {Day186/43:13-19}.
546) Brown {Day186/46:25}-{Day186/47:4}.
547) {LFB00104291}.
548) Brown {Day186/45:6-22}.
549) Brown {Day186/47:6-10}.
550) Stills from the programme are at {LFB00123288}; the accompanying trainer guide dated May 2013, is at {BAB00000058}.
551) Brown {Day186/146:17-24}.
552) Phase 1 Report Volume IV, paragraph 27.30.
553) Brown {Day186/202:22-25}; George {Day205/186:2-9}.
554) Roe {Day213/108:6-22}.
555) Smith {Day203/108:11-22}.
556) {LFB00091785}.
557) {LFB00091785/20}.
558) {LFB00091785/15}.
559) Brown {Day186/150:5}-{Day186/153:10}.
560) {LFB00032158/2}.
561) {LFB00042089/4}.
562) Brown {Day186/175:16}-{Day186/176:3}.
563) Brown {Day186/176:13-22}.
564) Brown {Day186/179:5-9}.
565) Brown {Day186/176:13}-{Day186/177:2}; {Day186/182:6-23}.
566) George {LFB00032823/17}, page 17, paragraph 69.
567) {LFB00042252/2}.
568) {LFB00032825}.
569) {LFB00032825}.
570) Brown {Day187/35:11}-{Day187/36:5}.
571) Brown {Day186/190:21}-{Day186/191:7}.
572) Brown {Day186/191:8-18}; {Day187/4:6-11}.
573) Brown {Day186/192:9-15}; Brown {LFB00123276/7} pages 6-7, paragraph 19.
574) {LFB00123288}; {BAB00000058}.
575) Brown {LFB00123276/8} page 8, paragraph 24.
576) {LFB00083388}.
577) Brown {Day187/9:19}-{Day187/10:3}.
578) George {LFB00032823/20} page 20, paragraphs 75-76; George {Day206/17:1-14}.
579) George {LFB00083884/19} page 19-20, paragraph 74.
580) Brown {Day187/12:13-16}; {Day187/13:7-13}.
581) {LFB00032160}; Brown {Day187/15:2-6}; {Day187/15:18-25}.
582) Brown {Day187/18:21-24}.
583) George {Day206/29:15}-{Day206/30:20}; {Day206/32:1-13}.
584) {LFB00001256/19}.
585) Documents created during and immediately after the Lakanal House inquests give conflicting views on whether radio testing formed a standard part of every s.7(2)(d) visit: {LFB00036836} and {LFB00098636/2}.
586) Brown {Day187/26:4}-{Day187/32:4}.
587) Johnson, Communications Report {CWJ00000119/110} paragraphs 5.4.4-5.4.5; Johnson {Day189/153:15}-{Day189/154:24}.
588) Johnson {Day189/155:2}-{Day189/156:1}; {Day189/156:13}-{Day189/157:16}.
589) Phase 1 Report Volume IV paragraph 27.1.
590) Phase 1 Report Volume IV paragraph 27.3.
591) {LFB00001255/7}.
592) {LFB00001256}.
593) {LFB00032783/6} paragraph 2.2.1.
594) Cowup {Day195/24:4-8}; Knight {Day245/146:10}-{Day245/148:11}.
595) {HOM00002128}.
596) {HOM00050078}.
597) Cowup {Day195/22:23}-{Day195/23:6}; {Day195/39:20}-{Day195/40:25}.
598) Cowup {Day195/20:9-19}.
599) Cowup {Day195/41:16-24}.
600) Cowup {Day195/91:4-16}.
601) Cowup {LFB00119849/37} page 37, paragraph 82.
602) Cowup {LFB00119849/51} page 51, paragraph 115.
603) Cowup {Day195/133:20}-{Day195/134:3}.
604) {LFB00033886/25}.
605) {LFB00033886/25}; {HOM00001124/4}; {LFB00001257/2} paragraph 2.2.
606) Cowup {Day195/113:4-18}.
607) Cowup {Day195/182:20-25}.
608) Cowup {Day195/187:7-19}; {LFB00102462}.
609) {LFB00102462/2}. Those amendments had in fact been suggested by GM Michael Curran, in an email sent to DAC Cowup on 18 March 2013 {LFB00090754}.
610) {LFB00001255/20}; {LFB00001256/14}.
611) {LFB00102462/3}.
612) {HOM00047743/2}.
613) Cowup {Day195/191:3}-{Day195/192:22}.
614) Cowup {Day195/195:18-23}. The draft GRA 3.2 was sent by Les Britzman, who was part of the Chief Fire and Rescue Adviser’s team, to Louise Upton, Peter Holland, Brian Martin, Dawn Eastmead, and others within DCLG, on 9 May 2013 {CLG00001921/2}.
615) Upton {Day248/61:22-24}; {Day248/100:4-7}.
616) {CLG00000624}.
617) {CLG10005807}.
618) Upton {Day248/85:3-19}.
619) Cowup {Day196/10:11-16}; {Day195/151:19}-{Day195/152:6}.
620) Upton {Day248/86:3-15}.
621) Cowup {Day196/12:1-11}.
622) Cowup {Day196/12:15-25}; {Day196/13:11-20}.
623) Cowup {Day196/14:2-19}.
624) Cowup {Day196/86:22}-{Day196/87:3}.
625) {LFB00102486/2}.
626) {LFB00052471}.
627) {LFB00034198/29}; {LFB00057988}.
628) {CLG00002780}.
629) {CLG00002781/16}.
630) Cowup {Day196/60:6-9}.
631) {CLG00002781/19-20}.
632) Cowup {Day196/106:2-10};{Day196/108:21}-{Day196/109:2}; {HOM00043991/3}.
633) Cowup {Day196/107:15-19}.
634) {HOM00043991/2}.
635) Phase 1 Report Volume IV paragraphs 27.2 and 27.3.
636) {LFB00102306}.
637) Cowup {LFB00119849/84} page 84, paragraph 187.
638) {LFB00102306/15}.
639) {LFB00102306/12}.
640) {LFB00085313}.
641) {LFB00086677}.
642) {LFB00085313}; Cowup {Day196/143:8}-{Day196/141:15}.
643) Cowup {Day196/146:18}-{Day196/147:9}; Utting {Day198/12:23}-{Day198/13:4}.
644) Cowup {Day196/147:15-20}; Utting {Day198/16:9-18}.
645) Utting {Day198/55:17}-{Day198/57:6}.
646) Utting {LFB00121173/2} page 2, paragraph 5; {LFB00121174}; {LFB00030368}; Utting {Day198/94:21}-{Day198/95:19}.
647) Phase 1 Report Volume IV paragraph 27.6.
648) Utting {Day198/47:21}-{Day198/48:16}.
649) Utting {Day198/66:3-12}.
650) The Inquiry received no evidence to indicate that any training had been developed for the 2015 edition of PN633, and neither DAC Cowup nor SM Utting were able to confirm otherwise: Cowup {Day197/29:18-23}; Utting {Day198/91:2-18}.
651) Roe {LFB00083834/7-8} pages 7-8, paragraphs 28 and 29.
652) {LFB00001255/19}.
653) Utting {Day198/60:13-25}-{Day198/61:2}.
654) Cowup {Day195/55:9-25}; {Day195/56:16-25}.
655) Utting {Day198/58:3-15}.
656) Dexter {LFB00032363/2} page 2, paragraphs 4 and 5.
657) Brown {LFB00032166/3-4} pages 3-4, paragraphs 5 and 9; George {LFB00032823/2} page 2, paragraph 6.
658) Lakanal Control Report {HOM00001124/7} paragraph 21.
659) Lakanal Control Report {HOM00001124/8} page 8, Chart 1.
660) Smith {LFB00121219/2-3} pages 2-3, paragraph 7. Following the fire, Joanne Smith was promoted to the rank of Deputy Assistant Commissioner and gave her evidence while holding that rank. At all material times she was a Senior Operations Manager and so, for clarity and consistency with the contemporaneous documentation, she will be referred to in that rank in this report.
661) Smith {LFB00121219/2-3} pages 2-3, paragraph 7, Smith {Day202/9:2-16}; Hayward statement {LFB00055191/17} page 17, paragraph 49.
662) Hayward {LFB00055191/17} page 17, paragraph 49; Lakanal Control Report {HOM00001124/8} paragraph 22.
663) SM Kelly’s training audit report {LFB00055220/4} paragraph 9.
664) The operation of the shifts and the impact of the shift system on the time available for training is covered in more detail below. The shift times and watch numbers, together with the minimum staffing numbers, are set out in tabular form in POM Hayward’s first witness statement: {LFB00055191/5} page 5, paragraphs 15-17
665) Hayward {LFB00055191/17-18} pages 17-18, paragraph 49. Smith {LFB00121219/3} page 3, paragraph 7.
666) Smith {Day202/13:22-24}.
667) Hayward {LFB00055191/18} page 18, paragraph 52.
668) Hayward {LFB00055191/17-18} pages 17-18, paragraph 49.
669) Smith {LFB00121219/3} page 2-3, paragraph 7.
670) Smith {LFB00121219/3} page 2-3, paragraph 7.
671) Smith {Day202/15:15-18}.
672) Smith {LFB00121219/3} page 3, paragraph 8.
673) Hayward {Day200/189:11-21}.
674) Bagnelle {LFB00122821/2} page 2, paragraph 6; Smith {LFB00121219/3} page 3, paragraph 8.
675) Hayward {LFB00055191/19-20} pages 19-20, paragraph 56-60.
676) Smith {LFB00121219/4} page 4, paragraph 9.
677) Smith {LFB00121219/4} page 4, paragraph 9.
678) Lakanal Control Report {HOM00001124/7} page 7, paragraph 19.
679) George {Day205/10:1-2}; George {LFB00032823/4} page 4, paragraphs 13 and 15.
680) George {Day205/11:3-16}.
681) George {LFB00032823/4} page 4, paragraph 16; George {Day205/15:6-11}.
682) George {Day205/22:1-5}.
683) George {Day205/21:2-10}.
684) George {Day205/21:11-23}.
685) George {Day205/4:20-22}.
686) George {LFB00032823/10} page 10, paragraph 39.
687) George {LFB00032823/10} page 10, paragraph 39.
688) George {LFB00032823/10} page 10, paragraphs 39 and 42.
689) George {Day205/108:19-23}.
690) George {Day205/108:21}-{Day205/109:4}. Hayward said that he left Brigade Control in July 2019: Hayward {Day199/5:1-3} and Hayward {LFB00086213/2} page 2, paragraph 7. Jonathan Smith {LFB00121171/4} page 4, paragraph 7.
691) Smith {LFB00121219/2} page 2, paragraph 6; Smith {Day202/6:8-15}.
692) Hayward {Day199/27:20-23}.
693) AC Chandler is recorded as attending or sending apologies to at least 6 meetings between 8 July 2012 and 9 November 2013. AC George is recorded as attending only part of the meeting on 8 March 2016 {LFB00123152/1} by way of an introduction to the staff.
694) George {Day205/13:2-5}.
695) Hayward {Day199/27:16-19}.
696) Hayward {Day199/32:19} – {Day199/33:1} and Hayward {Day199/50:20} – {Day199/51:13}.
697) Brown {Day206/42:19-25}.
698) See for example Principal Management Board Meeting draft minutes, 18 December 2013 {LFB00032168/5} where there the only involvement of Brigade Control is in relation to item 3.7 concerning the Lakanal Rule 43 Letter and item 4.3 regarding a report on a Radio MDT trial.
699) Brown {Day206/42:25}-{Day206/43:4}.
700) Brown {Day206/43:4-10}. As an example, AC Brown referred to meetings concerning the Vision mobilising system.
701) Hayward {Day199/37:16-18}; Brown {Day207/22:11-12}.
702) Brown {Day207/22:13-21}; Brown {Day207/11:4-20}.
703) The actions are set out in detail in the Lakanal Assurance Report {LFB00004801/12-15} Pre-Inquest actions 5 and 13.
704) Lakanal Assurance Report {LFB00004801/13-16} Pre-Inquest actions 8, 11, 12, 16 and 17.
705) Lakanal Assurance Report {LFB00004801/14} Pre-Inquest action 10.
706) Lakanal Assurance Report {LFB00004801/15} Pre-Inquest action 14.
707) Lakanal Assurance Report {LFB00004801/13} Pre-Inquest action 9.
708) Hayward {Day199/146:2-7}; Minutes of Lakanal House Board on 15 September 2010 {LFB00055192/7-8} Appendix 1; Brown {LFB00032166/5-6} pages 5-6, paragraph 14.
709) Brown {Day206/72:23-25}; Brown {LFB00084020/6} page 6, paragraph 10; Brown {Day206/73:6-16}. He was also received reports from DAC Cutbill who was a part of the Lakanal House action team: Brown {Day206/73:6-16}.
710) Brown {Day206/73:17-24}.
711) Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/12}; Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/7-24}.
712) Hayward {LFB00055191/6} page 6, paragraph 20, first bullet point; Hayward {LFB00086213/2-3} pages 2-3, paragraphs 10-12; Smith {LFB00121219/9} page 9, paragraph 20; Email from SOM Smith to DAC Cutbill, POM Hayward, Thomas Davies and GM Zymanczyk on 2 February 2010 {LFB00118272}.
713) Email from SOM Turner to DAC Cutbill and SM Hams copying in POM Hayward on 17 November 2009 {LFB00082629}; Email from SOM Turner to SM Hams on 19 November 2009 {LFB00075090}; Email from SOM Smith to DAC Cutbill, POM Hayward, Thomas Davies and GM Zymanczyk on 2 February 2010 {LFB00118272}.
714) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/7-24}; Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/12}.
715) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/7-24}.
716) Brown {Day206/79:5-9}; POM Hayward recalled that the gap analysis recommendations were accepted by the Lakanal House Board: {Day199/170:19-24}. However, the minutes of the meetings on 7 April, 5 May 2010 and 22 June 2010 do not make that clear: {LFB00060782/2}; {LFB00084028/3}; {LFB00055208/2-3}.
717) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/12} see ’Recommendations’.
718) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/8}; {HOM00001125/16} see ’Recommendations’.
719) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/23} see ’Recommendations’.
720) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/8}; {HOM00001125/11-20}; {HOM00001125/24}.
721) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/21}.
722) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/24}.
723) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/23}.
724) Smith {Day202/105:22-25}; Action Plan appended to the minutes of the meeting of the Lakanal House Board on 15 September 2010 {LFB00084031/8}; Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/13-14}.
725) FSC 54/04{LFB00055201/1}.
726) FSC 54/04{LFB00055201/1}.
727) FSC 54/04{LFB00055201/2-3}.
728) FSC 54/04{LFB00055201/2-3}.
729) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/10}.
730) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/7-12}.
731) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/7-8}.
732) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/8-9}.
733) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/9-10}.
734) Annex D of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/16-17}.
735) Emails between Michele McHugh (LFB) and Howard Jones (CLG) on 17 February 2010 {LFB00056548}. The minutes of the meeting of the Lakanal House Board on 5 May 2010 record that “It has been confirmed with CLG it is not intended that 54/04 supersede 10/93. However, it was noted that 10/93 was not on the CLG’s website, although it has now been confirmed as an extant document.” {LFB00084028/3}.
736) Hayward {Day199/158:25} – {Day199/159:1-2}; Smith {Day202/102:14-23}; Smith {LFB00121219/9} page 9, paragraph 21; Brown {Day206/82:14-18}.
737) Hayward {Day199/158:25}-{Day199/159:1-2}.
738) Hayward {Day199/158:9-18}.
739) Hayward {Day199/158:9-18}.
740) Smith {Day202/102:14-23}.
741) Brown {Day206/82:19-24}; Brown {Day206/88:18-21}; Dobson {Day211/140:12-20}.
742) Lakanal Control Report {HOM00001124/14} paragraph 61.
743) FSC 54/04{LFB00055201/2-3}; Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’{LFB00055201/10}.
744) Annex A of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/10}.
745) Hayward {Day199/158:9-18}.
746) Annex D of FSC 54/04 entitled ‘Emergency Call Management Protocol’ {LFB00055201/17}.
747) ‘Keeping People Safe’ training {LFB00118948/5}.
748) Two of the stated objectives of stage two of the emergency call-handling protocol were to “review assessment in light of further information” and to “continue to assess the call” {LFB00055201/8}. Annex D warned CROs that they might need to revisit stage one and two of the emergency call-handling protocol {LFB00055201/17}.
749) FSC 10/93{LFB00084051}; ‘Keeping People Safe’ training {LFB00118948/5}.
750) Email from DC Dexter to AC Brown on 14 January 2013 {LFB00085853/1}.
751) GM Lindridge’s review dated 4 January 2013 with DC Dexter and AC Brown’s comments {LFB00085854/5}.
752) Email from AC Brown to DC Dexter on 16 January 2013 {LFB00085853/1}.
753) GM Lindridge’s review dated 4 January 2013 with DC Dexter and AC Brown’s comments {LFB00085854/5}.
754) Brown {Day206/83:17-23}.
755) Lakanal Control Report dated November 2012 {HOM00001124/50} paragraph 295.
756) Brown {Day206/85:4-10}.
757) Brown {Day206/85:9-15}.
758) Brown {Day206/86:9-20}.
759) Hayward {Day199/164:5}-{Day199/165:1}.
760) GM Lindridge’s review dated November 2013, as amended in May 2014 {LFB00083988/8}.
761) Phase 1 Report Volume IV, paragraphs 29.45.e and 29.45.h.
762) FSC 10/93 {LFB00003617/1}.
763) ‘Keeping People Safe’ training {LFB00118948/6}.
764) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/11}.
765) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/11}.
766) PN539 dated 14 November 2007 {LFB00028382/20-21}.
767) Smith {Day202/119:13-20}.
768) PN539 dated November 2007 {LFB00028382/21}.
769) Phase 1 Report Volume IV, paragraph 29.45.f; Phase 1 Report Volume IV, paragraph 29.54.c.
770) Phase 1 Report Volume IV, paragraph 29.54.c.
771) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/14}.
772) PN539 dated 14 November 2007 {LFB00028382/20-21}.
773) Hayward {Day199/182:2-11}. SOM Smith could also not explain why: Smith {Day202/135:16-22}.
774) PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737}; Phase 1 Report Volume IV, paragraph 29.45.e.
775) Lakanal Control Report {HOM00001124/4} paragraph 1.
776) Lakanal Control Report {HOM00001124/4}.
777) Lakanal Control Report {HOM00001124/4} paragraph 3.
778) Lakanal Control Report {HOM00001124/4} paragraph 1.
779) Phase 1 Report Volume I, paragraphs 8.5-8.8.
780) Lakanal Control Report {HOM00001124/51-55} Chapter G.
781) Lakanal Control Report {HOM00001124/51-53}, paragraphs 303 to 309, Recommendations 1, 2, 3, 4, 5.
782) Lakanal Control Report {HOM00001124/51-53}, paragraphs 303 to 309, Recommendations 1, 2, 3, 4, 5.
783) Hayward {Day199/147:13} – {Day199/148:4}; Rule 43 Letter to Mr Ron Dobson, London Fire Commissioner dated 28 March 2013 {LFB00032158}.
784) Rule 43 Letter to Ron Dobson, London Fire Commissioner dated 28 March 2013 {LFB00032158/1}.
785) Phase 1 Report Volume IV, paragraph 29.5.
786) Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/14}.
787) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/8}; {HOM00001125/11-12}; {HOM00001125/16}; {HOM00001125/20}.
788) Action Plan appended to the minutes of the meeting of the Lakanal House Board on 15 September 2010 {LFB00084031/8}. The action was assigned to ‘AC/SD’, which meant “AC Service Delivery”, who was AC Brown at the time.
789) In both the version of PN539 dated 14 November 2007 that was current at the time of the Lakanal House fire {LFB00028382/1} and the version reviewed as current on 3 September 2010 {LFB00004735}, the ‘owner’ was designated as ‘Head of Service Delivery & Mobilising’.
790) Brown {Day206/91:2-6}. Hayward {Day199/193:10-13}; Brown {LFB00084020/6} page 6, paragraph 10; Brown {LFB00084020/11} page 11, paragraph 23.
791) Hayward {LFB00055191/7} page 7, paragraph 20.
792) Smith {LFB00121219/14} page 14, paragraph 34; Hayward {LFB00086213/5} page 5, paragraph 24; Emails between and Amelia Reynolds, Brigade Control Training Team Leader, POM Hayward, SOM Turner copying in SOM Smith between 13-21 July 2010 {LFB00057934}; Emails between SOM Smith and Amelia Reynolds between 2-3 September 2010 {LFB00109145}; Hayward {Day199/189:5}-{Day199/190:5}.
793) PN539 reviewed as current on 3 September 2010 {LFB00004735}.
794) Minutes of the Lakanal House Board meeting on 15 September 2010 {LFB00055192/2} item 5.15(1).
795) Smith did not recall the reviewed version of PN539 being presented to the Lakanal House Board: Smith {Day202/113:22}-{Day202/114:17}. There is no record of the updated policy being presented for approval at the meetings of the Lakanal House Board on 15 September 2010 {LFB00055192/2-3}, 8 November 2010 {LFB00084032/1} or 22 December 2010 {LFB00084033/2}, when the action was marked as completed. It ceased to be an agenda item thereafter.
796) SOM Smith did not think anyone had approved it: Smith {Day202/112:21-23}.
797) Brown {Day206/91:5-6}.
798) Brown {Day206/91:15-24}. SOM Smith said that the owner of the policy had ultimate responsibility for approving it, but in practice she did not think that had happened: Smith {Day202/111:22}-{Day202/112:1}.
799) SOM Smith did not think that anyone had approved it: Smith {Day202/112:21-23}. She said that she was not aware of anyone whose authority was required to make changes to PN539: Smith {Day202/110:23}-{Day202/111:6}.
800) As shown by the audit trail to PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737/22}.
801) PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737}.
802) Phase 1 Report Volume IV, paragraph 29.45.e.
803) Phase 1 Report Volume IV, paragraph 29.45.f.8.
804) Phase 1 Report Volume IV, paragraph 29.45.b.7.
805) Phase 1 Report Volume IV, paragraph 29.45.g.
806) Phase 1 Report Volume IV, paragraph 29.45.h.
807) PN539 dated 3 September 2010 {LFB00004735/16}; PN539 dated November 2007 {LFB00028382/20}.
808) PN539 dated 3 February 2011 {LFB00028601/16-17}.
809) PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737/16-17}.
810) Email from SOM Smith to POM Hayward on 3 February 2011 {LFB00109464}; Version of PN539 with tracked changes made by SOM Smith attached to her email to POM Hayward on 3 February 2011 {LFB00109465/17}.
811) Smith {Day202/137:5-8}.
812) Smith {Day202/137:8-12}.
813) Smith {Day202/137:12-15}.
814) Smith {Day202/137:8-17}.
815) Brown {Day206/99:3-22}.
816) Lakanal Control Report dated November 2012 {HOM00001124/50} paragraph 295.
817) Lakanal Control Report dated November 2012 {HOM00001124/52} paragraph 304.
818) Lakanal Control Report dated November 2012 {HOM00001124/52} paragraph 304.
819) Brown {Day206/102:4}-{Day206/103-4}.
820) GM Lindridge’s review dated 4 January 2013 {LFB00085854/6}.
821) GM Lindridge’s review dated 4 January 2013 {LFB00085854/6}.
822) Brown {Day206/95:6-18}.
823) Brown {Day206/94:22}-{Day206/95:5}.
824) PN539 dated 3 September 2010 {LFB00004735/16}.
825) PN539 dated 3 September 2010 {LFB00004735/16}.
826) PN539 dated 3 September 2010 {LFB00004735/16}.
827) PN539 dated 3 February 2011 {LFB00028601/16}.
828) PN539 dated 3 February 2011 {LFB00028601/16}.
829) Smith {Day202/124:12-22}.
830) Email from SOM Smith to POM Hayward on 3 February 2011 {LFB00109464}; Version of PN539 with tracked changes made by SOM Smith attached to her email to POM Hayward on 3 February 2011 {LFB00109465}; Emails between SOM Smith and POM Hayward on 3 February 2011 {LFB00058030}.
831) Smith {Day202/125:13}-{Day202/126:3}.
832) Phase 1 Report Volume IV, paragraph 29.49.c.
833) Lakanal Control Report dated November 2012 {HOM00001124/50} paragraph 293.
834) FSC 10/93 {LFB00003617/1} paragraph 2; ‘Keeping People Safe’ training {LFB00118948/6}.
835) GM Lindridge’s review dated 4 January 2013 {LFB00085854/13}.
836) GM Lindridge’s review dated 4 January 2013 {LFB00085854/13}.
837) PN539 dated 3 February 2011 {LFB00028601/16}; FSC 10/93 {LFB00003617/1} paragraph 2; ‘Keeping People Safe’ training {LFB00118948/6}.
838) PN539 dated 14 November 2007 {LFB00118944/20}.
839) PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737/16-17}.
840) Smith {Day203/13:24}-{Day202/14:4}.
841) Smith {Day203/14:3-5}.
842) Emails between and Amelia Reynolds, Brigade Control Training Team Leader, POM Hayward, SOM Turner copying in SOM Smith between 13-21 July 2010 {LFB00057934}; Emails between SOM Smith and Amelia Reynolds on 2-3 September 2010 {LFB00109145}; Hayward {Day199/189:5}-{Day199/190:5}.
843) Smith {Day203/14:13-16}.
844) Smith {Day203/15:3-7}.
845) Smith {Day203/14:5-9}; Smith {Day203/14:20-22}.
846) RIF for Operators approved on 12 March 2007 {LFB00121224/2}; RIF for Operators approved on 23 February 2011 {LFB00121240}.
847) RIF for Operators approved on 3 April 2014 {LFB00122837/2} paragraph 1.5. That was included following a report from a command unit training workshop with the control room: Bagnelle {LFB00122821/5} page 5, paragraph 15 and report {LFB00122833/2}.
848) Smith {Day203/16:14-22}.
849) Smith {Day203/16:22-25}.
850) Smith {Day203/17:1-13}.
851) FSC 54/04 {LFB00055201/17}.
852) Smith {Day203/17:14}-{Day203/18:3}.
853) Smith {Day203/17:14}-{Day203/18:3}; Phase 1 Report Volume IV, paragraph 29.76.
854) GM Lindridge’s review dated 4 January 2013 {LFB00085854/6}.
855) GRA 3.2 ‘Fighting fires – In high rise buildings’ dated February 2014 {LFB00001255}.
856) GRA 3.2 {LFB00001255/20}; GRA 3.2 {LFB00001255/29-31}; Cowup {Day195/64:4-8}; Cowup {Day195/99:1-5}
857) Email from Michele Kunneke to AC Brown and others on 10 May 2012 {LFB00093616}.
858) Brown {Day206/153:22}-{Day206/154:4}.
859) Brown {Day206/154:24}-{Day206/155:10}.
860) Smith {Day203/20:9-16}; Hayward {Day200/54:2-17}.
861) PN539 reviewed as current on 28 March 2014 and amended on 6 April 2017 {LFB00000737/22}.
862) Brown {Day206/109:20}-{Day206/110:2}.
863) Brown {Day206/110:13-16}.
864) Brown {Day206/110:3-25}.
865) Brown {Day206/110:19-21}.
866) Lakanal Assurance Review dated August 2018 {LFB00004801/13}.
867) Lakanal Assurance Review dated August 2018 {LFB00004801/14}.
868) Hayward {LFB00055191/7} page 7, paragraph 20; Smith {LFB00121219/11} page 11, paragraph 26; Smith {Day203/26:11}-{Day203/28:7}.
869) Smith {Day203/26:11-24}.
870) Smith {LFB00121219/11} page 11, paragraph 26; Smith {Day203/26:11-24}.
871) Smith {LFB00121219/12} page 12, paragraph 27; Email from SOM Smith to all Brigade Control Staff on 23 February 2011 {LFB00121237}; RIF for Operators approved on 23 February 2011 {LFB00121240}; RIF for Supervisors approved on 23 February 2011 {LFB00111192}.
872) Smith {LFB00121219/12} page 12, paragraph 28.
873) Smith {LFB00121219/12} page 12, paragraph 28.
874) Smith {LFB00121219/12} page 12, paragraph 28; RIF for Operators approved on 23 February 2011 {LFB00121240/10-19}.
875) Smith {Day202/105:22-25}.
876) RIF for Operators approved on 23 February 2011 {LFB00121240/24}; RIF for Supervisors approved on 23 February 2011 {LFB00111192/5}; Smith {Day203/26:25}-{Day203/27:4}.
877) Smith {Day203/27:5}-{Day203/28:17}.
878) Minutes of Lakanal House Board meeting on 15 September 2010 {LFB00055192/2} item 5.6; Minutes of Lakanal House Board meeting on 4 February 2011 {LFB00055215/2} item 5.5; Smith {Day202/28:14-20}.
879) Email from AOM Bonnett to SOM Smith, SOM Turner, AOM Sharp and AOM O’Shea on 27 June 2011{LFB00028381/1-2}.
880) Email from AOM Bonnett to SOM Smith, SOM Turner, AOM Sharp and AOM O’Shea on 27 June 2011{LFB00028381/3}.
881) Email from AOM Bonnett to SOM Smith, SOM Turner, AOM Sharp and AOM O’Shea on 27 June 2011{LFB00028381/3-4}.
882) Email from SOM Smith to POM Hayward on 27 June 2011{LFB00028381/1}.
883) Smith {Day203/29:16}-{Day203/30:24}; Smith {Day203/34:3}-{Day203/35:8}; Smith {LFB00121219/13} page 13, paragraphs 30-31; Smith {MET00080606/20}.
884) Email from SOM Smith to all Brigade Control Staff on 23 February 2011 {LFB00121237/1}.
885) Smith {Day203/30:25}-{Day203/32:5}.
886) Brigade Control training records 2011-2018 {LFB00041763} columns Y, Z and AA.
887) Bagnelle {LFB00122821/5} page 5, paragraphs 14-15; Email from AOM Bonnett to SOM Bagnelle on 10 January 2013 {LFB00122822/2-3}.
888) Bagnelle {LFB00122821/5} page 5, paragraph 15; RIF for Operators approved on 18 February 2013 {LFB00122835}; RIF for Supervisors approved on 18 February 2013 {LFB00122836}.
889) GM Lindridge’s Review dated 4 January 2013 {LFB00085854/5}; Email from GM Lindridge to SOM Bagnelle, POM Hayward, AC Brown and others on 9 January 2013 {LFB00118958/1}; Email from SOM Bagnelle to OST on 11 January 2013 {LFB00122822/2}; Email from AOM Bonnett to all Brigade Control staff on 18 February 2013 {LFB00055234/1}; Bagnelle {LFB00122821/6} page 6, paragraph 17.
890) Smith {LFB00121219/12} page 12, paragraph 28; RIF for Operators approved on 18 February 2013 {LFB00122835}; RIF for Supervisors approved on 18 February 2013 {LFB00122836}.
891) Bagnelle {LFB00122821/5} page 5, paragraph 15.
892) Email from AOM Bonnett to all Brigade Control staff on 18 February 2013 {LFB00055234/1}; RIF for Operators approved on 18 February 2013 {LFB00122835}; RIF for Supervisors approved on 18 February 2013 {LFB00122836}.
893) Email from AOM Bonnett to all Brigade Control staff on 18 February 2013 {LFB00055234/1}.
894) Brigade Control training records 2011-2018 {LFB00041763}; Hayward {LFB00055191/27} paragraph 77.
895) Bagnelle {LFB00122821/5-6} pages 5-6, paragraph 14-16; RIF for Operators approved on 3 April 2014 {LFB00003542}.
896) RIF for Operators approved on 3 April 2014 {LFB00003542}.
897) Bagnelle {LFB00122821/5} page 5, paragraph 14; RIF for Supervisors approved on 3 April 2014 and updated on 2 April 2016 {LFB00003541}.
898) RIF for Supervisors approved on 3 April 2014 and updated on 2 April 2016 {LFB00003541}.
899) Phase 1 Report Volume IV, paragraph 29.49.
900) Phase 1 Report Volume IV, paragraph 29.50.
901) RIF for Operators approved on 23 February 2011 {LFB00121240/14}.
902) Smith {Day203/70:17-20}.
903) Smith {Day203/70:21}-{Day203/71:1}.
904) Smith {Day203/71:2-14}.
905) Smith {Day203/71:2-14}.
906) Smith {LFB00121219/15} page 15, paragraph 36.
907) Smith {Day203/69:24}-{Day203/70:6}.
908) Smith {Day203/70:3-10}; Smith {Day203/71:15}-{Day203/72:8}.
909) RIF for Operators approved on 23 February 2011 {LFB00121240/14-15}.
910) RIF for Operators approved on 23 February 2011 {LFB00121240/15}.
911) Smith {Day203/73:1-3}.
912) RIF for Operators approved on 18 February 2013 {LFB00122835}; RIF for Operators approved on 3 April 2014 {LFB00003542}.
913) GM Lindridge’s Review dated 4 January 2013 {LFB00085854/5}; Email from GM Lindridge to SOM Bagnelle, POM Hayward, AC Brown and others on 9 January 2013 {LFB00118958/1}; Email from SOM Bagnelle to OST on 11 January 2013 {LFB00122822/2}; Email from AOM Bonnett to all Brigade Control staff on 18 February 2013 {LFB00055234/1}; Bagnelle {LFB00122821/6} page 6, paragraph 17.
914) Bagnelle {LFB00122821/5} page 5, paragraph 15.
915) Reports from command unit training workshops {LFB00122833/1}.
916) Report from command unit training workshops {LFB00122833/1}.
917) Report from command unit training workshops {LFB00122833/2}.
918) RIF for Operators approved on 3 April 2014 {LFB00003542}.
919) Phase 1 Report Volume IV, paragraph 29.54.c and paragraph 29.60.
920) Gap Analysis {LFB00004750/10-11}.
921) Gap Analysis {LFB00004750/11}.
922) Gap Analysis {LFB00004750/11}.
923) Smith {Day202/105:22-25}.
924) RIF for Operators approved on 23 February 2011 {LFB00121240/17}.
925) RIF for Operators approved on 23 February 2011 {LFB00121240/17}.
926) RIF for Operators approved on 23 February 2011 {LFB00121240/17}.
927) Email from SOM Smith to AOM Bennett and AOM Suarez copying in POM Hayward on 3 January 2011 {LFB00033220}.
928) Email from SOM Smith to AOM Bennett and AOM Suarez copying in POM Hayward on 3 January 2011 {LFB00033220/1}.
929) See also Smith {LFB00121219/16} page 16, paragraph 39.
930) Draft RIF for Operators dated 16 November 2010 as edited by SOM Smith {LFB00083530/15}.
931) Smith {Day203/78:10-24}.
932) Smith {Day203/78:22}-{Day203/79:2}.
933) RIF for Operators approved on 18 February 2013 {LFB00122835}; RIF for Supervisors approved on 18 February 2013 {LFB00122836}; RIF for Operators approved on 3 April 2014 {LFB00003542}; RIF for Supervisors approved on 3 April 2014 and updated on 2 April 2016 {LFB00003541}.
934) Phase 1 Report Volume IV, paragraph 29.54.c.
935) See, for example, email from SOM Smith to SM Utting on 23 January 2011 {LFB00028301}; Email from SOM Smith to POM Hayward on 24 January 2011 {LFB00058020}; Utting {LFB00118918/3} page 3, paragraph 8; Smith {Day203/128:20}-{Day203/129:7}.
936) Draft version of PN155 dated 10 February 2011 {LFB00083447/4} paragraph 6.6.
937) Smith {LFB00121219/26} page 26, paragraph 69; Smith {Day203/91:4}-{Day203/92:12}.
938) Smith {Day203/92:22}-{Day203/93:12}.
939) PN790 issued on 23 February 2012 and reviewed as current on 17 April 2014 {LFB00001257/5} paragraph 8.7.
940) Smith {Day203/94:19}-{Day203/95:7}.
941) Smith {Day203/94:19}-{Day203/95:7}.
942) Hayward {Day199/220:8-21}.
943) Smith {Day203/96:9-16}.
944) Smith {Day203/96:17}-{Day203/97:6}.
945) Smith {Day203/97:20-25}; Smith {MET00080606/13}.
946) Hayward {Day199/221:10-23}.
947) GRA 3.2 {LFB00001255/19}.
948) Email from Michele Kunneke to all ACs on 13 April 2011 {LFB00033332/1}.
949) Brown {Day206/120:9-22}.
950) Brown {Day206/120:9}-{Day206/121:4}
951) Brown {Day206/121:2-4}
952) Phase 1 Report Volume IV, paragraph 29.99
953) Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/15}.
954) Lakanal House Assurance Review dated 7 August 2018 {LFB00004801/15}.
955) Hayward {Day199/194:8-11}; Smith {LFB00121219/10} page 10, paragraph 24.
956) Minutes of Lakanal House Board meeting on 20 April 2011 {LFB00084035/1} item 4.4.
957) Minutes of Lakanal House Board meeting on 30 November 2011 {LFB00084038/2} item 8.1.
958) Minutes of the Lakanal House Board meeting on 12 December 2011 {LFB00084039/2} item 8.1; Dobson {Day211/143:19}-{Day211/144:1}.
959) Email from Linda Armstrong to Sue Marshall copying Commissioner Dobson and DAC Cutbill dated 3 February 2012 {LFB00100551}. Draft Letter to DCLG dated 23 December 2011 {LFB00004744}.
960) Letter from Ron Dobson to Sir Ken Knight dated 3 February 2012 {LFB00004728}.
961) Letter from Ron Dobson to Sir Ken Knight dated 3 February 2012 {LFB00004728}.
962) Smith {Day202/143:17-24}.
963) Smith {Day 202/144:1-11}.
964) Smith {Day202/144:22}-{Day202/144:3}.
965) Minutes of the Lakanal House Board meeting on 2 July 2012 {LFB00084043/1} item 5.1; Minutes of Lakanal House Board meeting on 7 September 2012 {LFB00084044/1} item 4.1; Minutes of Lakanal House Board meeting dated 17 October 2012 {LFB00084045/2} item 6.1; Hayward {Day199/194:17-25}.
966) Lakanal Control Report dated November 2012 {HOM00001124/51} paragraph 303.
967) Minutes of the Lakanal House Board meeting on 19 November 2012 {LFB00084046/1} item 6.1.
968) Minutes of the Lakanal House Board meeting on 14 December 2012 {LFB00040033/1}; Dobson {Day211/144:23}-{Day211/145:1}.
969) Dobson {Day211/145:2-6}.
970) Dobson {Day211/145:7-15}.
971) Minutes of Lakanal House Board meeting on 30 September 2013 {LFB00050644/1} item 5.1.
972) Dobson {Day211/148:15-19}.
973) There is nothing dealing with those issues in the coroner’s rule 43 letter to DCLG dated 28 March 2013 {CLG00000401} nor in her rule 43 letter to the LFB dated 28 March 2013 {LFB00032158}.
974) Dobson {Day211/148:3}-{Day211/149:5}.
975) GM Lindridge’s review dated 4 January 2013 {LFB00085854/5}.
976) GM Lindridge’s review dated 4 January 2013 with DC Dexter and AC Brown’s comments {LFB00085854/5}.
977) Annex B to Lakanal Control Report entitled ‘Comparison between national guidance and LFB policy and training’ {HOM00001125/14}; {HOM00001125/17}.
978) Brown {Day206/99:6-13}.
979) Brown {Day206/100:4-12}.
980) Email from AC Brown to AC Chandler on 4 April 2013 {LFB00028942/1}.
981) Email from AC Chandler to AC Brown on 28 June 2013 {LFB00060701}.
982) Hayward {Day199/200:2-5}.
983) Phase 1 Report Volume IV, paragraph 29.42.
984) Phase 1 Report Volume IV, paragraph 29.45(b).
985) Smith {Day202/153:4} – {Day202/154:25}.
986) Smith {Day202/154:7-13}.
987) Smith {Day202/154:14-15}.
988) Smith {Day202/156:18} – {Day202/157:12}.
989) Smith {Day202/183:18} – {Day202/185:22}.
990) Smith {Day202/183:18} – {Day202/185:22}.
991) For example, see Smith {Day202/183:18} – {Day202/185:22}.
992) Daily Bulletin {LFB00109347/3}.
993) SOM Smith reported that four fire survival guidance calls had been received {Day202/185:14-22}; the ‘End of Incident Report’ suggested that approximately eight fire survival guidance calls had been received because of the number of fire survival guidance messages transferred from the control room to the incident ground {LFB00123671/3-8}. The figure of 17 fire survival guidance calls was contained in a comment to a draft of PN155 at paragraph 6.2 {LFB00109485/3}.
994) Debrief proforma for Adair Tower {LFB00035092/3}; FSG Database {LFB00031757} rows 20 to 28.
995) Smith {Day202/201:1-20}.
996) Lakanal Control Report {HOM00001124/35-37}, Table 4, rows 4, 28, 31, 38 & 43.
997) Hayward {LFB00121176/16} page 16, paragraph 66; Bagnelle {LFB00122821/2} page 2, paragraph 6 and {LFB00122821/6} page 6, paragraph 19.
998) Smith {LFB00121219/12-13} pages 12-13, paragraph 29.
999) Smith {Day202/162:5} – {Day202/163:12}.
1000) Hayward {LFB00121176/16} page 16, paragraph 66; Bagnelle {LFB00122821/2} page 2, paragraph 6 and {LFB00122821/6} page 6, paragraph 19; Smith {LFB00121219/17} page 17, paragraph 43.
1001) Smith {Day202/183:18-24}.
1002) Smith {Day202/183:18-24}.
1003) SOM Smith reported that four fire survival guidance calls had been received {Day202/185:14-22}; the end of incident report suggested that between seven and eight fire survival guidance calls had been received {LFB00123671}; the figure of 17 fire survival guidance calls was recounted in a comment to a draft of PN155 at paragraph 6.2 {LFB00109485/3}.
1004) {Day202/185:14-22}.
1005) Email from Andy Hickmott to Scott Hayward, Dave Brown, Peter Cowup, Rita Dexter and Ron Dobson titled “FW: Daily Bulletin.12-11-10.doc” dated 12 November 2010 {LFB00110785/2}.
1006) Brown {Day206/126:9-16}.
1007) Brown {Day206/126:1-7}.
1008) Brown {Day206/126:8-9}.
1009) Brown {Day206/126:17} – {Day206/127:11}.
1010) Brown {Day206/126:17} – {Day206/127:11}.
1011) Email from Andy Roe to numerous LFB participants {LFB00033345/1-4}.
1012) Email from Andy Roe to numerous LFB participants {LFB00033345/1-4}.
1013) Email from Andy Roe to numerous LFB participants {LFB00033345/1-4}.
1014) Smith {Day202/171:3-10}; Hayward {Day199/210:11-20}.
1015) ‘Feedback: High Rise and FSG Policies Test Exercise 16 June 2011 Southwark’ {LFB00033384/11}; Smith {Day202/172:1-18}.
1016) Smith {Day202/176:23} – {Day202/177:10}; Hayward {Day199/212:21} – {Day199/214:7}.
1017) Minutes of debrief meeting {LFB00056628}.
1018) Smith {Day202/173:20} – {Day202/173:24}; Feedback: High Rise and FSG Policies Test Exercise 16 June 2011 Southwark’ {LFB00033384/11}.
1019) Hayward {Day199/212:7-12}; Feedback: High Rise and FSG Policies Test Exercise 16 June 2011 Southwark {LFB00033384/10}; Minutes of debrief meeting {LFB00056628}.
1020) Feedback: High Rise and FSG Policies Test Exercise 16 June 2011 Southwark {LFB00033384/10-11}. No witness was able to identify that incident.
1021) Minutes of debrief meeting {LFB00056628/4}.
1022) Hayward {Day199/215:12-21}.
1023) Hayward {Day199/215:12-21}.
1024) Utting {Day198/103:10-25}; Smith {LFB00121219/26} page 26, paragraph 69.
1025) Draft PN155 issue date 10 February 2011 {LFB00111471/5}
1026) Brown {Day206/122:23} – {Day206/123:11}; Smith {Day202/198:3} – {Day202/199:7}; Patrick Utting could not recall having discussed or even having considered the possibility of more than 5 fire survival guidance calls being generated by a single incident or how the control room would manage such an occurrence: Utting {Day198/118:17} – {Day198/119:18}.
1027) GRA 3.2 {LFB00001255/3}.
1028) GRA 3.2 {LFB00001255/30}.
1029) Smith {Day202/199:8-19} and {Day203/20:3-8}; Hayward {Day200/53:13} – {Day200/54:22}.
1030) Smith {Day202/199:20} – {Day202/200:3}; Hayward {Day200/53:13} – {Day200/54:22}.
1031) Phase 1 Report Volume IV, paragraph 29.40.
1032) Harrington {LFB00102245/8} page 8, paragraph 18; Withers {LFB00084123/5} page 5, paragraph 16; Minutes of Fire Survival Guidance Meeting on 12 March 2014 {LFB00084124}.
1033) Harrington {LFB00102245/12} page 12, paragraph 31.
1034) Harrington {LFB00102245/12} page 12, paragraph 31.
1035) Withers {LFB00084123/5} page 5, paragraph 16.
1036) FSG Database {LFB00031757}.
1037) Debrief proforma for Adair Tower {LFB00035092/5}; FSG Database {LFB00031757}; Smith {Day202/201:1-20}.
1038) Smith {Day202/205:6-18}.
1039) Smith {Day202/206:18} – {Day202/207:14}. The FSG Database did not record any lessons to be learnt or systems to be reviewed {LFB00031757}. The Incident Debrief form did not record any learning about fire survival guidance management {LFB00035092}. The IMP report for the incident did not record any learning about fire survival guidance management {MET00080621}.
1040) {LFB00035092/5}. It should be noted that on 20 December 2016, following a command unit training exercise, Liz Hymns expressed concern that a whiteboard had not been set up for managing multiple fire survival guidance calls to enable the control room to manage the information, even though she considered that to be standard practice: {LFB00052219/1}.
1041) Phase 1 Report Volume IV paragraphs 29.49-29.50.
1042) Hayward {Day199/36:21}-{Day199/37:15}; George {Day205/12:3-6}; Brown {Day206/156:13-17}.
1043) Hayward {Day199/37:16}-{Day199/38:3}; George {Day205/152:5}-{Day205/153:24}.
1044) Brown {Day206/156:10-17}.
1045) Hayward {LFB00086213/7} page 7, paragraph 38; Hayward {Day199/38:4-8}.
1046) Hayward {Day199/33:21}-{Day199/34:1}; Hayward {LFB00055191/17} page 17, paragraph 48; Smith {LFB00121219/6} page 6, paragraph 15.
1047) Hayward {Day199/34:2-7}.
1048) Hayward {LFB00055191/7} page 7, paragraph 20; {LFB00055191/17} page 17, paragraph 47; Hayward {Day199/38:9-13}.
1049) Hayward {LFB00086213/8} page 8, paragraph 39.
1050) Hayward {Day199/32:6-14}; {Day199/51:6-24}.
1051) Hayward {Day199/51:6-24}.
1052) Hayward {Day199/32:15-21}; {Day199/51:6-24}.
1053) Hayward {Day199/32:15-21}; {Day199/34:5-14}.
1054) Hayward {Day199/118:17-19}; PN164 amended on 28 January 2009 {LFB00084054/3} paragraph 2.5; PN164 reviewed as current on 6 May 2015 {LFB00084054/8} paragraphs 2.5-6.
1055) Hayward {Day199/34:19}-{Day199/35:3}.
1056) Hayward {Day199/32:19}-{Day199/33:17}; {Day199/50:20-24}.
1057) Hayward {Day199/32:19}-{Day199/33:1}; {Day199/51:6-13}.
1058) Hayward {Day199/32:19}-{Day199/33:1}.
1059) Hayward {LFB00055191/18} page 18, paragraph 52.
1060) Hayward {LFB00055191/17} page 17, paragraph 49.
1061) Hayward {LFB00055191/17} page 17, paragraph 48; Hayward {LFB00055191/25} page 25, paragraph 72; Training Spreadsheet {LFB00055223}.
1062) Hayward {LFB00055191/24} page 24, paragraph 68.
1063) Lakanal Assurance Report {LFB00004801/13-14}.
1064) Lakanal Control Report {HOM00001124/13-16} paragraphs 49-74.
1065) Fire Service Circular {LFB00003617/1} paragraph 6.
1066) Fire Service Circular {LFB00003617/2} paragraph 7.
1067) Fire Service Circular {LFB00003617/6}.
1068) Lakanal Control Annexures {LFB00004750/37}.
1069) Lakanal Control Annexures {LFB00004750/28}; Hayward {Day200/120:14}-{Day200/121:25}.
1070) Lakanal Control Annexures {LFB00004750/28}.
1071) Hayward {LFB00121176/3-4} pages 3-4, paragraphs 13 and 14; Lakanal House Assurance Review {LFB00004801/14}. Further training was developed for new entrants {LFB00107484}.
1072) Refresher training presentation on building types and concepts (2011) {LFB00086228}.
1073) Fire Survival Guidance presentation {LFB00028265}.
1074) Fire Survival Training: Introduction to Fire and Human Behaviour presentation, dated March 2010 {LFB00119961}.
1075) Smith {LFB00121219/18} page 18, paragraph 47; Smith {Day203/191:10-16}.
1076) Hayward {LFB00055191/25} page 25, paragraph 74; Minutes of Lakanal House Board Meeting of 15 September 2010 {LFB00055192/1}.
1077) Hayward {Day200/79:9}-{Day200/80:16}; {Day200/80:19-23}; Hayward {LFB00055191/24} page 24, paragraph 69.
1078) Minutes of Lakanal House Board Meeting of 15 September 2010 {LFB00055192/2} item 5.6; Hayward {LFB00055191/6-7} pages 6-7, paragraph 20.
1079) Minutes of Lakanal House Board Meeting of 15 September 2010 {LFB00055192/1} item 5.4.
1080) Email from Scott Hayward to Chris Sharp, Lindsay Turner, Joanne Stibbards and Robin Hannan dated 23 February 2010 regarding Fire Survival Planning Meeting 22nd February 2010 {LFB00028258/1}.
1081) Hayward {LFB00121176/6} page 6, paragraph 20.
1082) Hayward {LFB00121176/6} page 6, paragraph 20; Hayward {Day200/127:22}-{Day200/128:19}.
1083) Hayward {LFB00121176/6} page 6, paragraph 20.
1084) 2010 FSG Training {LFB00028265}; 2011 FSG Training {LFB00086214}; Hayward {Day200/96:12} – {Day200/97:11}; Building Types and Concepts presentation {LFB00086228}; Hayward {Day 200/107:3-20}; Fire and Human Behaviour Training presentation, dated March 2010 {LFB00119961}; Hayward {Day200/111:2}-{Day200/112:7}.
1085) Smith {Day203/202:7-11}.
1086) 2011 FSG Training {LFB00086214/1}.
1087) Hayward {Day200/112:9-14}.
1088) Fire Service Circular {LFB00003617/1} paragraph 2.
1089) 2010 FSG Training {LFB00028265/19-28}.
1090) Smith {Day203/200:5}-{Day203/201:25}.
1091) 2010 FSG Training {LFB00028265}; 2011 FSG Training {LFB00086214/21}.
1092) Hayward {Day200/102:2-24}; {Day200/108:13}-{Day200/110:1}.
1093) Hayward {Day200/104:2-16}; FSG Refresher Presentation {LFB00086214/15-16}; 2010 FSG Training {LFB00028265}.
1094) 2010 FSG Training {LFB00028265}; 2011 FSG Training presentation {LFB00086214/21}.
1095) Hayward {Day200/116:24}-{Day200/118:1}.
1096) Smith {Day204/49:20}-{Day204/50:2}.
1097) Comments on FSG {LFB00083547/1}.
1098) Smith {Day204/65:11-15}.
1099) FSG Brigade Control Training presentation (2012) {LFB00086226}; Smith {Day204/42:4}-{Day204/48:12}.
1100) Smith {Day204/42:4-19}.
1101) Smith {Day204/42:4-19}.
1102) Audit of Quality Management Systems Fire Survival Training Course dated 3 August 2010 {LFB00109082}.
1103) Audit of Quality Management Systems Fire Survival Training Course dated 3 August 2010 {LFB00109082/6} paragraph 40.
1104) Audit of Quality Management Systems Fire Survival Training Course dated 3 August 2010 {LFB00109082/11}.
1105) Hayward {Day200/131:22}-{Day200/132:22}.
1106) Hayward {LFB00055191/26} page 26, paragraph 75; 2011 FSG Role Play scenario 1 {LFB00055226} 2011 FSG Role Play scenario 2 {LFB00055227}; 2011 FSG Role Play scenario 3 {LFB00003788}; 2011 FSG Role Play scenario 4 {LFB00003682}.
1107) Hayward {Day200/131:22}-{Day200/132:22}.
1108) Lakanal Control Report {HOM00001124/52} paragraph 308.
1109) Minutes of Lakanal House Board Meeting 15 September 2010 {LFB00055192/2}; Minutes of Lakanal House Board Meeting 15 November 2010 {LFB00055213/1}.
1110) Minutes of Lakanal House Board Meeting 15 September 2010 {LFB00055192/2}.
1111) Fire Service Circular {LFB00003617/6}; Lakanal Control Annexures {LFB00004750/37}.
1112) Fire Service Circular {LFB00003617/3} paragraph 11.
1113) Fire Service Circular {LFB00003617/3} paragraph 11.
1114) Smith {Day204/13:23}-{Day204/14:6}.
1115) Brown {Day207/59:8-11}.
1116) Hayward {LFB00055191/24} page 24, paragraph 68. Minutes of Lakanal House Board Meeting of 22 June 2010 {LFB00055208}; Minutes of Lakanal House Board Meeting of 15 September 2010 {LFB00055192}; Minutes of Lakanal House Board Meeting of 8 November 2010 {LFB00055213}.
1117) Hayward {Day200/143:8-19}; Smith {Day204/19:6-12}.
1118) Hayward {Day200/147:16}-{Day200/148:3}.
1119) Hayward {Day200/157:3-6}.
1120) Hayward {Day200/147:16}-{Day200/148:3}.
1121) Hayward {Day200/154:24}-{Day200/155:2}.
1122) Brown {Day207/64:7-17}.
1123) Minutes of Lakanal House Board Meeting of 22 June 2010 {LFB00055208}; Minutes of Lakanal House Board meeting of 15 September 2010 {LFB00055192}; Minutes of Lakanal House Board Meeting of 8 November 2010 {LFB00055213}; Hayward {Day200/148:19-23}.
1124) Minutes of Lakanal House Board Meeting of 8 November 2010 {LFB00055213/6}; Brown {Day207/64:1}-{Day207/65:8}.
1125) Brown {Day207/61:16}-{Day207/63:4}.
1126) Brown {Day207/62:8-21}.
1127) Smith {Day204/21:8-25}.
1128) Hayward {Day200/149:3-11}.
1129) Smith {Day204/23:20-24}.
1130) Smith {Day204/25:4-12}.
1131) Lakanal Control Report {HOM00001124/53}.
1132) Hayward {Day200/154:24}-{Day200/155:5}.
1133) Email from Scott Hayward to Lindsay Turner and Joanne Stibbards dated 31 May 2011 regarding Fire Survival Refresher Package {LFB00058087/1}; Hayward {Day200/180:15-25}.
1134) Hayward {Day200/154:24}-{Day200/155:25}; Hayward {LFB00055191/10} page 10, paragraph 21.8.
1135) Hayward {Day200/155:6}-{Day200/157:15.
1136) Hayward {Day200/167:6-16}; FSG Training Record {LFB00041763}.
1137) Hayward {Day200/162:17}-{Day200/163:3}; Hayward {LFB00055191/26} page 26, paragraph 75; Hayward {Day200/184:14-17}.
1138) Hayward {Day200/162:10-16}.
1139) Hayward {Day200/162:17}-{Day200/163:3}; Hayward {LFB00055191/26} page 26, paragraph 75.
1140) Hayward {LFB00055191/26} page 26, paragraph 74.
1141) Hayward {LFB00055191/26} page 26, paragraph 75.
1142) Hayward {Day200/168:16-22}.
1143) Hayward {Day200/171:15-17}.
1144) Hayward {LFB00086213/14} page 14, paragraph 73; Email from Chris Sharp to Natalie Bagnelle, Vic Bagnelle, Sam Coaker, Scott Hayward, David Hughes, Steve Perry, Joanne Stibbards and Lindsay Turner dated 27 September 2012 {LFB00060696}.
1145) Hayward {LFB00086213/14} page 14, paragraph 73; Hayward {LFB00055191/24} page 24, paragraph 69; Hayward {Day200/190:6-11}.
1146) Hayward {LFB00086213/14} page 14, paragraph 74; Email from Victor Bagnelle to Scott Hayward regarding Control Report {LFB00122840/1}.
1147) Hayward {Day200/192:8-15}.
1148) Hayward {LFB00055191/24} page 24, paragraph 70.
1149) Hayward {LFB00055191/24} page 24, paragraph 70.
1150) Hayward {Day200/195:24}-{Day200/196:6}.
1151) Hayward {Day200/196:10-24}.
1152) Hayward {LFB00055191/24-25} pages 24-25, paragraph 71.
1153) Hayward {Day200/197:4-10}.
1154) Hayward {Day200/195:24}-{Day200/196:6}; Hayward {LFB00055191/24} page 24, paragraphs 69-71.
1155) Email from Chris Sharp to Natalie Bagnelle, Vic Bagnelle, Sam Coaker, Scott Hayward, David Hughes, Steve Perry, Joanne Stibbards and Lindsay Turner dated 27 September 2012 {LFB00060696}.
1156) Hayward {Day200/218:1}-{Day200/219:5}.
1157) Hayward {LFB00055191/24} page 24, paragraph 69; Email from Thomas Davies to Scott Hayward dated 5 February 2013 {LFB00060872/4}; Email from Scott Hayward to Vic Bagnelle dated 7 February 2013 {LFB00039935/1-2}; Bagnelle {LFB00122821/12} page 12, paragraphs 41-43.
1158) Hayward {LFB00055191/24-25} pages 24-25, paragraph 71.
1159) Email chain with Scott Hayward, Chris Sharp, Nicola O’Shea and Vic Bagnelle dated 6 February 2013 {LFB00122840/3-4}.
1160) Hayward {Day200/205:19}-{Day200/206:14}.
1161) Hayward {Day200/205:19}-{Day200/206:14}.
1162) Email from Scott Hayward to Vic Bagnelle dated 7 February 2013 {LFB00039935/1}; Hayward {Day200/208:9}-{Day200/209:19}.
1163) Email from Scott Hayward to Vic Bagnelle dated 7 February 2013 {LFB00039935/1}.
1164) Brown {Day207/82:4}-{Day207/83:3}.
1165) Email from Dave Brown to Scott Hayward dated 9 February 2013 {LFB00060872}; Brown {Day207/78:7-14}.
1166) Hayward {LFB00055191/24} page 24, paragraph 69; Bagnelle {LFB00122821/12} page 12, paragraphs 41-43; Email from Scott Hayward to Vic Bagnelle dated 7 February 2013 {LFB00122840/2}; Hayward {Day200/209:16-25}; Brown {Day207/78:7-14}.
1167) Hayward {LFB00055191/24} page 24, paragraph 69; Bagnelle {LFB00122821/12} page 12, paragraphs 41-43; Email from Scott Hayward to Vic Bagnelle dated 7 February 2013 {LFB00122840/2}; Hayward {Day200/209:16-25}; Brown {Day207/78:7-14}.
1168) Hayward {LFB00055191/26-29} pages 26-29, paragraphs 67.5 and 69; Hayward {Day201/15:20}-{Day202/16:8}.
1169) Hayward {Day200/188:7-25}.
1170) Hayward {Day200/190:22}-{Day200/191:10}.
1171) Brown {LFB00032166/21} page 21, paragraph 65; Brown {LFB00084020/10} page 10, paragraph 20; Brown {Day207/43:21-24}. Email chain between Scott Hayward, Lindsay Turner and Joanne Stibbards dated 22 February 2012 {LFB00058256/1-2}.
1172) This was accepted by AC Brown. Brown {LFB00084020/10} page 10, paragraph 20.
1173) Brown {Day207/43:21-24}; Brown {Day207/48:25} – {Day207/49:8}; Brown {LFB00032166/21} page 21, paragraph 65.
1174) Brown {LFB00032166/21} page 21, paragraph 65.
1175) Brown {LFB00032166/21} page 21, paragraph 65; Brown {LFB00084020/10} page 10, paragraph 20.
1176) Brown {Day207/46:13-21}.
1177) Brown {LFB00032166/21} page 21, paragraph 65.
1178) Brown {LFB00084020/10} page 10, paragraph 20.
1179) Brown {Day207/47:25}-{Day207/48:18}; Hayward {Day201/8:15}-{Day201/9:7}.
1180) Hayward {LFB00055191/26-29} pages 26-29, paragraphs 77 to 78.4; Hayward {Day201/16:6-8}; Smith {Day204/87:19}-{Day204/88:4}.
1181) Hayward {LFB00055191/26-29} pages 26-29, paragraphs 77 to 78.4; Hayward {Day201/16:6-8}; Joanne Smith {LFB00121219/23} page 23, paragraph 60; Smith {Day204/110:23}-{Day204/111:16}.
1182) Hayward {LFB00055191/28} page 28, paragraph 78.2.2.
1183) Smith {Day204/123:7-20}; Brown {Day207/109:10-24}.
1184) Hayward {LFB00055191/28} page 28, paragraph 78.2.2; Smith {Day204/123:7-25}; {Day204/132:1-9}; Minutes of Operational Review Team Meeting on 11 January 2017 {LFB00040541/2}; Brown {Day207/109:10-24}.
1185) Smith {LFB00121219/24} page 24, paragraph 62; Smith {Day204/113:23}-{Day204/116:12}.
1186) Hayward {LFB00055191/29} page 29, paragraph 78.3; Hayward {LFB00086213/7} page 7, paragraph 35; Hayward {Day201/80:13}-{Day201/84:8}.
1187) Hayward {Day200/110:24-25}.
1188) Smith {Day204/116:17-23}.
1189) Smith {Day204/117:11-22}.
1190) Brown {Day207/105:15}-{Day207/106:25}.
1191) Hayward {LFB00055191/26} page 26, paragraph 74.
1192) Hayward {LFB00055191/26} page 26, paragraph 74.
1193) Hayward {LFB00055191/26-29} pages 26-29, paragraph 74 and paragraph 78.4; Smith {Day204/91:13-21}.
1194) Hayward {Day201/16:9-22}.
1195) Hayward {LFB00055191/30} page 30, paragraph 79; Hayward {Day201/17:12-18}.
1196) Hayward {LFB00055191/30} page 30, paragraph 79; Hayward {Day201/17:12-18}.
1197) Smith {LFB00121219/6} page 6, paragraph 15.
1198) Smith {LFB00121219/22} page 22, paragraph 56; Smith {Day204/79:22}–{Day204/80:15}.
1199) Smith {Day204/79:9-20}.
1200) Smith {Day204/78:3-18}.
1201) Smith {Day204/81:13}-{Day204/82:10}.
1202) Smith {Day204/83:1-6}.
1203) Smith {Day204/81:17-20}.
1204) Smith {Day204/84:1-15}.
1205) Smith {LFB00121219/25} page 25, paragraph 68; Smith {Day204/96:7-21}.
1206) Smith {Day204/96:22}-{Day204/98:9}.
1207) Smith {Day204/91:22}-{Day204/92:7}.
1208) Smith {Day204/92:4-7}.
1209) Brown {Day201/21:22}-{Day201/22:4}; Hayward {Day201/73:12-25}.
1210) Draft LFB Report ‘Review of the Lakanal Action Plan’ {LFB00085854/14} and {LFB00085854/26}. See comment “d10”.
1211) Draft LFB Report ‘Review of the Lakanal Action Plan’ {LFB00085854/14} and {LFB00085854/26}. See comment “d10”; Hayward {LFB00055191/25} page 25, paragraph 74.
1212) Brown {Day207/72:14-22}; Brown {LFB00032166/21} page 21, paragraph 66.
1213) Email from Chandler to Brown dated 28 June 2013 regarding Lakanal Audit {LFB00060701/1}.
1214) Email from Chandler to Brown dated 28 June 2013 regarding Lakanal Audit {LFB00060701/1}.
1215) Email from Chandler to Brown dated 28 June 2013 regarding Lakanal Audit {LFB00060701/1}; Hayward {Day201/29:8-19}.
1216) Hayward {Day201/30:1-10}.
1217) Email from Brown to Bevan copied to Scott Hayward, Philip Evans and Danielle Cotton dated 3 July 2014 regarding HSE info – control training {LFB00037428/1-2}.
1218) Email from Brown to Bevan copied to Scott Hayward, Philip Evans and Danielle Cotton dated 3 July 2014 regarding HSE info – control training {LFB00037428/2}.
1219) Hayward {Day201/31:8}-{Day201/32:16}.
1220) Hayward {Day201/35:11-22}.
1221) Email from Brown to Bevan copied to Scott Hayward, Philip Evans and Danielle Cotton dated 3 July 2014 regarding HSE info – control training {LFB00037428/1-2}.
1222) Brown {Day207/92:1-14}; Brown {LFB00084020/13} page 13, paragraph 29.
1223) Hayward {Day201/55:6-24}.
1224) Brown {LFB00084020/13} page 13, paragraph 30; Hayward {Day201/55:22}-{Day201/57:14}; Brown {Day207/94:15-20}.
1225) Email chain between Scott Hayward and Karen Mason dated 17-18 November 2014 regarding Brigade Control Audit {LFB00030108}; Hayward {Day201/42:1-4}; Internal Audit – Progress Report Quarter 3 2014/2015 dated 9 March 2015 {LFB00044640/1}.
1226) Brown {Day207/94:10}-{Day207/95:16}.
1227) Review of Brigade Control Report dated July 2016 {LFB00032826}; George {LFB00083884/11} page 11, paragraph 34; George {Day205/55:6}-{Day205/57:6}.
1228) Review of Brigade Control Terms of Reference {LFB00032827/1}.
1229) Review of Brigade Control – the issues raised by staff prior to the review commencing {LFB00032831/3}; George {Day205/36:13-20}; George {LFB00032823/4} page 4, paragraphs 12 and 13.
1230) George {Day205/55:6-14}.
1231) George {Day205/57:3-6}.
1232) George {Day205/65:4-8}.
1233) George {Day205/65:9}-{Day205/67:3}.
1234) George {Day205/80:8-19}.
1235) George {Day205/151:6-25}.
1236) George {Day205/151:6-25}; George {Day205/153:16-24}.
1237) George {Day205/151:20}-{Day205/153:5}.
1238) George {LFB00032823/8} page 8, paragraph 31; George {LFB00083884/14} page 14, paragraph 49.
1239) CMB report on Review of Brigade of Control for CMB, dated 15 February 2017 {LFB00032824/6}.
1240) Hayward {Day201/75:2}-{Day201/76:3}.
1241) George {Day205/165:9-22}.
1242) George {Day205/165:9-22}.
1243) George {Day205/165:23}-{Day205/166:10}; {Day205/169:23}-{Day205/170:2}.
1244) Lakanal Control Report {HOM00001124/53}; Lakanal Control Report {HOM00001124/31} paragraphs 161-163.
1245) Lakanal Control Report {HOM00001124/53}; Lakanal Control Report {HOM00001124/31} paragraphs 161-163.
1246) Brown {Day207/28:5-20}.
1247) Brown {Day207/28:21}-{Day207/29:5}.
1248) Smith {Day202/49:11-15}.
1249) Call Coach Management Note {LFB00121231/6}; Smith {Day202/31:10}-{Day202/32:23}.
1250) Call Coach Management Note {LFB00121231/2-3}; Smith {Day202/34:1-23}.
1251) Call Coach Management Note {LFB00121231/2-3}.
1252) Call Coach Management Note {LFB00121231/4}.
1253) Smith {LFB00121219/7} page 7, paragraph 17.
1254) Smith {Day202/35:10-14}; {Day202/45:10}-{Day202/47:11}.
1255) Smith {Day202/38:1-18}; The detail required to assess a fire survival guidance call was not included in the call-handling excellence standard, Call Coach Management Note {LFB00121231} Appendix B; Smith {Day202/38:11-18}.
1256) Smith {Day202/39:4-13}; {Day202/59:15-21}.
1257) Smith {Day202/38:19-22}.
1258) Hayward {Day199/56:22}-{Day199/57:17}; see SOM Smith’s comments on the draft training audit report prepared by SM Kelly {LFB00109082/9}; Smith {Day202/41:25}-{Day202/43:13}.
1259) Hayward {Day199/58:1-10}.
1260) Smith {Day202/37:3-16}; Brown {Day207/27:9-17}.
1261) Hayward {LFB00055191/39} page 39, paragraph 96.
1262) Hayward {LFB00055191/39} page 39, paragraph 97; Hayward {Day199/59:15-19}.
1263) Smith {Day202/47:10-12}.
1264) Smith {Day202/50:15-25}.
1265) Smith {Day203/9:2-21}.
1266) Smith {Day203/10:13-19}; FSG Database {LFB00031757}.
1267) Smith {Day203/11:6-14}.
1268) The FSG Database did not record any lessons to be learnt or systems to be reviewed {LFB00031757}.
1269) Smith {LFB00121219/8} page 8, paragraph 18; Smith {Day202/50:13}-{Day202/51:12} and {Day202/52:20-23}.
1270) Smith {LFB00121219/8} page 8, paragraph 18; Smith {Day202/54:4}-{Day202/55:6}; {Day202/54:7}-{Day202/57:6}.
1271) Smith {LFB00121219/8} page 8, paragraph 18; Hayward {Day199/64:16}-{Day199/65:5}; Smith {Day202/49:16-20}.
1272) Hayward {Day199/62:21-25}; SOM Smith also thought that Peter Suarez, Control Commander in the Technical Support Group, also listened to the call {Day202/52:15-19}.
1273) Hayward {Day199/63:22-24} and {Day199/65:10-12}. The only email about feedback after a fire survival guidance call review provided to the Inquiry was: Email from Joanne Stibbards to Keith Diamond dated 22 October 2011 {LFB00121235}.
1274) Email from Joanne Stibbards to Keith Diamond dated 22 October 2011 {LFB00121235}.
1275) Smith {Day202/62:21-24}.
1276) Hayward {Day199/64:3-7}.
1277) Smith {Day202/64:10-24}.
1278) Smith {LFB00121219/8} page 8, paragraph 19; Smith {Day202/66:7-17}.
1279) Smith {LFB00121219/8} page 8, paragraph 19; Smith {Day202/69:3-14}.
1280) Smith {Day202/69:15-18}.
1281) Smith {Day202/69:19}-{Day202/70:9}.
1282) Fire Survival Guidance Calls (PN790) {LFB00001257}; It was designed to complete Pre-Inquest action 14, Lakanal Assurance Report {LFB00004801/15}; For the Phase 1 findings in respect of PN790, Phase 1 Report Volume IV paragraphs 29.18 – 29.23, 29.47 and 29.48.
1283) Utting {LFB00118918/3} page 3, paragraph 8; Smith {Day203/129:12-14}; {Day203/155:16-23}; Smith {MET00080606/13}.
1284) Smith {MET00080606/13}.
1285) Utting {LFB00118918/3} page 3, paragraph 8; Smith {Day203/128:20}-{Day203/129:7}.
1286) Fire Survival Guidance Calls (PN790) {LFB00001257} paragraphs 4.1, 5.13, 6.2, 7.6 and 9.4, and Appendix 3.
1287) Brown {Day206/124:3-19}.
1288) Hayward {Day206/124:3-19}.
1289) Hayward {LFB00121176/6} page 6, paragraph 21: Hayward {Day199/223:3}-{Day199/224:10}.
1290) Training Spreadsheet {LFB00055223}; AOM Christine Sharp and AOM Gary Court were provided with training “Fire Survival Guidance calls – 790” but there is no other training recorded about PN790 in respect of any other control staff member. There was no training for PN790 recorded on the Control FSG Training Record {LFB00041763}.
1291) Training Spreadsheet {LFB00055223}; AOM Christine Sharp and AOM Gary Court were provided with training “Fire Survival Guidance calls – 790” but there is no other training recorded in respect of PN790. There was no training for PN790 recorded on the Control FSG Training Record {LFB00041763}; Hayward {Day199/224:25}-{Day199/225:7}.
1292) Fire Survival Guidance Calls (PN790) {LFB00001257/5} paragraph 8.7.
1293) Smith {MET00080606/13}.
1294) Hayward {Day199/221:10-14}; Smith {MET00080606/13}.
1295) Smith {MET00080606/13}; Smith {Day203/97:7-25}.
1296) Hayward {Day199/221:15-23}.
1297) Email from Andy Roe to numerous LFB participants {LFB00033345/1-4}.
1298) Minutes of the Heygate Estate high-rise exercise de-brief meeting {LFB00056628/4}; Feedback: High Rise and FSG Policies Test Exercise 16th June 2011 Southwark {LFB00033384/11}.
1299) Hayward {Day199/213:24}-{Day199/214:7}.
1300) Hayward {Day199/213: 24}-{Day199/214:7}; Smith {Day202/172:1-16}.
1301) Feedback: High Rise and FSG Policies Test Exercise 16th June 2011 Southwark {LFB00033384/11}; Minutes of the Heygate Estate high-rise exercise de-brief meeting {LFB00056628/4}; Hayward {Day199/214:15-23}.
1302) Exercise Florian Facilitator Briefing {LFB00122827/5}; Bagnelle {LFB00122821/15} page 15, paragraph 55.
1303) Hayward {Day200/4:16}-{Day200/5:2}; Fire Survival Guidance Calls (PN790) {LFB00001257/1}.
1304) Brown {Day206/134:9-18}.
1305) Brown {Day206/135:8-15}.
1306) Brown {Day206/135:16}-{Day206/136:9}.
1307) Brown {Day206/134:9-18}; Exercise Florian Facilitator Briefing {LFB00122827/5}.
1308) This is also recognised by Vic Bagnelle in an email dated 5 November 2013 regarding Exercise Penfold {LFB00050721/1}.
1309) Email from David Lindridge to Dave Brown, Patrick Utting, Martin Corbett, Scott Hayward and Victor Bagnelle dated 9 January 2013 {LFB00118958/1}.
1310) Hayward {Day200/14:11}-{Day200/15:24}.
1311) Hayward {LFB00055191/28} page 28, paragraph 78.2.2.
1312) Brief for Exercise Penfold {LFB00122841}; Bagnelle {LFB00122821/14} paragraphs 51-53.
1313) Email chain between Paul Trew and Scott Hayward and Vic Bagnelle dated 27 June 2013 {LFB00050487/2}.
1314) Bagnelle {LFB00122821/14} page 14, paragraph 52.
1315) Bagnelle {LFB00122821/14} page 14, paragraph 52.
1316) Scott Hayward could not assist, Hayward {Day200/42:9-24}.
1317) Feedback from N O’Shea following Exercise Penfold {LFB00122826/2}.
1318) Hayward {Day200/48:1-4}.
1319) Lakanal Assurance Report {LFB00004801/16}.
1320) Hayward {LFB00055191/8} page 8, paragraph 20; Hayward {Day201/94:18-23}; Supervisor FSG Training Presentation {LFB00086222}.
1321) Supervisor FSG Training Presentation {LFB00086222/7}.
1322) Supervisor FSG Training Presentation {LFB00086222}.
1323) Supervisor FSG Training Presentation {LFB00086222/7-10}.
1324) Hayward {Day201/99:16-22}; Supervisor FSG Training Presentation {LFB00086222/13}.
1325) Supervisor FSG Training Presentation {LFB00086222/9}.
1326) Hayward {Day201/98:8-16}.
1327) Supervisor FSG Training Presentation {LFB00086222/9}; Hayward {Day201/99:23}-{Day201/102:25}.
1328) Smith {Day204/150:18}-{Day204/153:1}.
1329) Bagnelle {LFB00122821/17} page 17, paragraph 62; Supervisor FSG Training Powerpoint {LFB00122832}.
1330) Supervisor FSG Training Powerpoint {LFB00122832/5}.
1331) Supervisor FSG Training Powerpoint {LFB00122832/13}.
1332) There is no reference to it in Scott Hayward’s witness statements or in the Control FSG Training Record {LFB00041763}; Training Spreadsheet {LFB00055223} does record that a number of supervisors received various forms of fire survival guidance training between 2014 and 2017.
1333) Hayward {Day201/103:21}-{Day201/104:6}; Real {MET00080520/6-9}; May {MET00080506/16-17}.
1334) Hayward {Day201/118:21}-{Day201/119:9}.
1335) Smith {Day202/174:24-25}.
1336) Jonathan Smith {LFB00121171/9} page 9, paragraph 24.
1337) Jonathan Smith {LFB00121171/10} page 10, paragraph 30; AC Smith’s ‘Control: Overview and Control Improvement Plan’ {LFB00084097/11}.
1338) George {Day205/17:16-19}; AC George recalled the control centres being located at Wembley, Croydon and Lewisham.
1339) George {Day205/17:19-24}.
1340) LFB Lakanal Control Report {HOM00001124/26} paragraph 132. George ‘Review of Brigade Control’ July 2016 {LFB00032826/4} paragraph 13.
1341) George {Day205/18:7-9}.
1342) George {Day205/75:6-8}; LFEPA Self-assessment 2015 – LGA Peer Challenge {LFB00047742/56}.
1343) George {Day205/82:11-18}.
1344) Training Audit Recommendations 15 January 2013 {LFB00106102/2}.
1345) Smith {Day202/93:5-8}.
1346) George {Day205/82:21-23}.
1347) George {Day205/85:7-9}.
1348) Hayward {Day199/125:5-18}.
1349) Hayward {Day199/127:22}-{Day199/128:1}.
1350) LFB Report ‘How Training Works’ {LFB00055127/5} paragraph 2.7.
1351) LFB Report ‘How Training Works’ {LFB00055127/5} paragraph 2.7.
1352) Hayward {Day201/123:10-12}.
1353) SM Kelly report {LFB00055220/9} paragraphs 63-64 and 66-68.
1354) Smith {Day202/38:1-7}.
1355) Email from AC Chandler to AC Brown, 28 June 2013 {LFB00060701/2} item 16.
1356) Brown {Day207/121:2-3}.
1357) Hayward {Day201/129:16-22}.
1358) Review of Brigade Control July 2016 {LFB00032826/11-13} paragraph 49; Brown {Day207/120:25}-{Day207/121:12}.
1359) Review of Brigade Control July 2016 {LFB00032826/11} paragraph 49(b).
1360) George {LFB00083884/7} page 7, paragraph 29(b).
1361) George {LFB00083884/12} page 12, paragraph 40 and George {LFB00083884/6} page 6, paragraph 29(b).
1362) George {LFB00083884/13} page 13, paragraphs 41-42.
1363) SM Kelly’s Report of Training Audit {LFB00055220/4} paragraph 9.
1364) Hayward {Day199/28:25}–{Day199/29:9}.
1365) Smith {Day202/73:2-18}.
1366) Smith {Day202/98:17-18}
1367) LFB Report ‘How Training Works’ {LFB00055127/23} paragraphs 7.1; Groves {LFB00102138/44} page 44, paragraph 81.
1368) Hayward {Day199/20:7-12}.
1369) Hayward {Day199/20:10-17}.
1370) Brown {LFB00032166/5} page 5, paragraph 13.
1371) Hayward {LFB00055191/11} page 11, paragraph 26.
1372) Hayward {LFB00055191/12} page 12, paragraph 29.
1373) Hayward {LFB00055191/111-12} pages 111-112, paragraph 27.
1374) Hayward {LFB00055191/19} page 19, paragraph 56.
1375) Hayward {LFB00055191/20} page 20, paragraphs 59-60; George {Day205/7:4-5}.
1376) George {Day205/19:16-19}.
1377) George {Day205/19:19-22}.
1378) Hayward {LFB00055191/13} page 13, paragraph 35.
1379) Hayward {LFB00055191/13} page 13, paragraph 33.
1380) George {Day205/20:4-12}.
1381) George {Day205/20:12}; {Day205/20:2-4}.
1382) Hayward {LFB00055191/21} page 21, paragraph 63.
1383) Brown {Day207/89:8}; Hayward {Day201/56:12-25}.
1384) Smith {Day202/74:12-15}.
1385) Smith {Day 202/74:22-25}.
1386) Smith {Day204/93:19-24}.
1387) Smith {LFB00121219/23} page 23, paragraph 61.
1388) Hayward {Day201/63:21-24}.
1389) Hayward {Day201/63:25}-{Day201/64:2}.
1390) Hayward {LFB00055191/18} page 18, paragraph 49.
1391) Hayward {LFB00055191/18} page 18, paragraph 51.
1392) Brigade Control Management Meeting Minutes 8 December 2015 {LFB00123099/2}.
1393) JCC Meeting Minutes {LFB00123113/7}.
1394) George {Day205/95:12-21}.
1395) George {Day205/20:19-23}.
1396) Hayward {LFB00055191/26} page 26, paragraph 74 (table).
1397) Hayward {Day201/52:2-5}.
1398) Brown {LFB00084020/13} page 13, paragraph 30.
1399) Brown {LFB00084020/13} page 13, paragraph 30.
1400) Brown {Day207/93:7-17}.
1401) George {Day205/80:8-14}.
1402) Hayward {Day200/15:7-15}.
1403) George {LFB00032823/11} page 11, paragraph 46; George {LFB00083884/14-15} pages 14-15, paragraph 50.
1404) George {Day 205/173:16-20}.
1405) Hayward {Day201/16:23}–{Day201/17:2}.
1406) Hayward {Day201/17:12-18}.
1407) Hayward {Day201/129:16-22}.
1408) Review of Brigade Control, July 2016 {LFB00032826/11-13} paragraph 49; Brown {Day207/120:25}-{Day207/121:12}.
1409) {LFB00058876/2}.
1410) Real {MET00080520/14} page 14, paragraph 4; Hayward {LFB00055191/18} page 18, paragraph 52; Hayward {Day199/50:2-6}; Smith {Day202/95:9-13}; George {Day205/111:10-12}; Brown {Day206/160:3-7}.
1411) Fire Service Manual Volume 1: Fire Service Technology, Equipment and Media Communications and Mobilising {INQ00014945/129}.
1412) Review of Brigade Control, July 2016 {LFB00032826/9} paragraph 39; Hayward {LFB00055191/18} page 18, paragraph 52.
1413) Review of Brigade Control, July 2016 {LFB00032826/11} paragraph 49.
1414) Review of Brigade Control, July 2016 {LFB00032826/9} paragraph 39.
1415) Brown {Day206/66:18-24}; {Day206/157:19-20}.
1416) Control - Overview and Control Improvement Plan, dated 22 July 2019 {LFB00084097/4}.
1417) Control - Overview and Control Improvement Plan, dated 22 July 2019 {LFB00084097/4}.
1418) Tables setting out the minimum numbers of staff required from 2011, Hayward {LFB00055191/5} page 5, paragraphs 15-17.
1419) Smith {Day202/95:9-13}.
1420) Hayward {Day199/43:19-21}.
1421) Hayward {Day199/49:9}-{Day199/50:1}.
1422) George {Day205/111:23-25}.
1423) Fire Service Manual Volume 1: Fire Service Technology, Equipment and Media Communications and Mobilising {INQ00014945/129}.
1424) Smith {Day204/23:12-24}; Real {MET00080520/14} page 14, paragraph 4.
1425) Hayward {Day199/47:1-8}.
1426) Hayward {Day199/43:2-5}.
1427) Hayward {Day199/43:6-7}.
1428) Hayward {Day200/80:19}-{Day200/81:1}.
1429) Hayward {Day200/81:2-10}.
1430) Smith {Day202/97:23}-{Day202/98:5}.
1431) Smith {Day204/24:4}-{Day204/25:3}.
1432) Smith {Day204/127:20}-{Day204/128:16}; Hayward {LFB00055191/28} page 28, paragraph 78.2.
1433) Review of Brigade Control - the issues raised by staff prior to the review commencing {LFB00032831/2} paragraph 3a; George {Day205/52:7}-{Day205/53:6}.
1434) Review of Brigade Control {LFB00032826/11} paragraph 49.
1435) Hayward {Day199/47:4-6}; Hayward {Day199/87:11-13}; Brown {Day206/40:25}-{Day206/41:1}; George {Day205/53:25}-{Day205/54:3}.
1436) George {Day205/114:5-7}.
1437) George {Day205/114:22-25}.
1438) Lakanal Control Report dated November 2012 {HOM00001124/26} paragraphs 130 and 134 and {HOM00001124/31} paragraph 167.
1439) Gap Analysis dated 7 April 2010 {HOM00001125/23}; SM Kelly’s draft audit of Brigade Control training dated August 2010 {LFB00055203/7} paragraphs 46-49.
1440) AC Jonathan Smith’s briefing note titled ‘Control – Overview and Control Improvement Plan’ dated 22 July 2019 {LFB00084097/3}.
1441) Fire Service Circular {LFB00003617/3} paragraph 11.
1442) Appendix 1 of the Fire Service Manual 1: Fire Service Technology, Equipment and Media, Communications and Mobilising (Published 1998) entitled ‘Control Staff – Training, Competence and Promotion’ {INQ00014945/129}.
1443) PN164 as issued on 29 September 1994 and amended on 28 January 2009 {LFB00084054/3}.
1444) That was the case for all of its subsequent revisions. PN164 reviewed as current on 6 May 2015, which was the version in force on 14 June 2017 {LFB00084054/11}.
1445) Hayward {Day199/77:16}-{Day199/79:11}; Hayward {Day199/121:22-25}; Brown {Day207/4:15-25}; Minutes of the Lakanal House Board Meeting on 22 June 2010 {LFB00055208/3} item 8.8; Minutes of the Lakanal House Board Meeting on 21 July 2010 {LFB00055210/3} item 7.5; Minutes of the Lakanal House Board meeting on 15 September 2010 {LFB00084031/2} item 5.10.
1446) Hayward {Day199/77:16}-{Day199/79:11}.
1447) George {Day205/82:7-20}.
1448) Minutes of the Lakanal House Board Meeting on 8 November 2010 {LFB00055213/1}; Hayward {Day199/123:8-23}.
1449) Brown {Day206/163:2-17}.
1450) Minutes of the Brigade Control Management Meeting held on 18 July 2012 {LFB00113237/7-8} item 5.
1451) Brown {LFB00032166/3-4} pages 3-4, paragraph 7.
1452) Hayward {Day199/85:23}-{Day199/86:2}.
1453) Hayward {Day199/78:13}-{Day199/79:2}; Hayward {Day199/123:1-3}.
1454) Hayward {Day199/126:6-9}; {Day199/78:23}-{Day199/79:2}; George {Day205/86:22}-{Day205/87:5}.
1455) Hayward {Day199/126:12-22}.
1456) Hayward {Day199/126:12-22}.
1457) Minutes of the Brigade Control Management Meeting on 12 September 2012 {LFB00113402/6} item 5.
1458) Hayward {Day199/96:17-21}.
1459) Minutes of the Brigade Control Management Meeting on 12 September 2012 {LFB00113402/6} item 5.
1460) GM Lindridge’s Review dated 4 January 2013 {LFB00033943/14}.
1461) GM Lindridge’s Review dated 4 January 2013 {LFB00033943/14}.
1462) Hayward {Day199/104:15-17}.
1463) Hayward {Day199/104:18-23}.
1464) Hayward {Day199/125:3-18}; {Day199/126:24}-{Day199/127:15}; {Day199/131:9-18}; Hayward {LFB00055191/23} page 23, paragraph 67; Brown {Day207/6:23}-{Day207/7:14}.
1465) Hayward {Day199/127:16-24}; {Day199/131:5-8}; Hayward {LFB00055191/23} page 23, paragraph 67.
1466) Hayward {Day199/127:16}-{Day199/128:3}.
1467) Brown {Day207/8:6-14}.
1468) Brown {Day207/7:18-23}; {Day207/8:15-25}.
1469) Brown {Day207/8:15-25}.
1470) Email from AC Brown to AC Chandler on 4 April 2013 {LFB00028942/2}.
1471) Brown {Day206/170:15-24}.
1472) Brown {Day206/170:25}-{Day206/171:2}.
1473) Brown {Day206/171:3-9}.
1474) Email from POM Hayward to OM Vic Bagnelle on 9 May 2013 {LFB00042081/1}.
1475) Email from AC Chandler to AC Brown on 28 June 2013 {LFB00060701/1}.
1476) Email from AC Chandler to AC Brown on 28 June 2013 {LFB00060701/2}.
1477) Email from POM Hayward to SOM Bagnelle, SOM Diamond and Tejinder Ajimal on 22 July 2014 {LFB00051294}.
1478) Smith {Day204/160:2-5}.
1479) Smith {Day204/160:2-10}; {Day204/161:1-4}.
1480) Smith {Day204/160:2-10}; {Day204/161:1-4}; {Day204/166:1-6}.
1481) Smith {Day204/165:13-19}.
1482) Smith {Day204/162:23}-{Day204/163:4}; {Day204/166:25}-{Day204/167:3}.
1483) Email chain between Scott Hayward and Karen Mason dated 17-18 November 2014 regarding Brigade Control Audit {LFB00030108}; Hayward {Day201/42:1-4}; Internal Audit – Progress Report Quarter 3 2014/2015 dated 9 March 2015 {LFB00044640/1}.
1484) Hayward {Day201/42:1-4}.
1485) Email from Karen Mason to SOM Bagnelle on 14 November 2014 {LFB00030108/3}.
1486) Summary of MOPAC Audit of Brigade Control dated February 2015 {LFB00044640/25-26}.
1487) Summary of MOPAC Audit of Brigade Control dated February 2015 {LFB00044640/25-26}.
1488) Hayward {Day201/45:19}-{Day201/47:2}; Brown {Day207/87:6-18}.
1489) Brown {Day207/88:18-25}.
1490) Hayward {Day201/51:17}-{Day201/52:18}.
1491) AC George Review of Brigade Control dated July 2016 {LFB00032826/11} paragraph 47.
1492) AC George Review of Brigade Control dated July 2016 {LFB00032826/12} paragraphs 49 c-f.
1493) Appendix 2 to AC George’s Review of Brigade Control dated July 2016 {LFB00032826/31}; George {Day205/105:15-25}.
1494) George {Day205/100:23}-{Day205/101:1}.
1495) George {Day205/101:2-19}.
1496) George {LFB00083884/6} page 6, paragraph 29(b); George {Day205/104:12}-{Day205/105:7}; Hayward {Day199/133:16-18}; Hayward {Day199/143:23-25}.
1497) Email from POM Hayward to AC George on 7 November 2016 {LFB00083865/9}; George {LFB00083884/6} page 6, paragraph 29(b); Smith {Day204/182:12}-{Day204/184:17}; Hayward {Day199/113:13}-{Day199/114:1}; George {Day205/106:7-14}.
1498) Brown {Day206/173:6-17}; George {Day205/82:7}-{Day205/84:14}; {Day205/86:6-15}; Hayward {Day199/110:2-24}.
1499) George {Day205/83:3-4}.
1500) AC Smith’s briefing note entitled ‘Control – Overview and Control Improvement Plan’ dated 22 July 2019 {LFB00084097/3-4}.
1501) Review of Brigade Control, July 2016 {LFB00032826/5} paragraph 22.
1502) George {Day205/69:14-17}; London Safety Plan 2014 {LFB00032107/70}.
1503) Review of Brigade Control, July 2016 {LFB00032826/5} paragraph 22.
1504) Hayward {Day199/15:22}-{Day199/16:7}; Brown {Day206/47:2-13}.
1505) Brown {Day206/46:24-25}.
1506) Brown {Day206/46:21-24}.
1507) Brown {Day206/45:23}-{Day206/46:15}.
1508) George {Day205/71:9-21}.
1509) George {Day205/71:11-21}.
1510) George {Day205/71:23}-{Day206/72:3}.
1511) Summary of MOPAC Audit of Brigade Control dated February 2015 {LFB00044640/25}.
1512) Minutes of Brigade Control Management Meeting on 18 July 2012 {LFB00113237/7-8} item 5; Minutes of Brigade Control Management Meeting on 12 September 2012 {LFB00113402/6} item 5; Email from POM Hayward to OM Vic Bagnelle dated 9 May 2013 {LFB00042081/1}.
1513) Email from AC Chandler to AC Brown dated 28 June 2013 {LFB00060701/2}.
1514) Email from POM Hayward to SOM Bagnelle, OM Diamond and SM Ajimal on 22 July 2014 {LFB00051294}.
1515) AC George’s Review of Brigade Control dated July 2016 {LFB00032826/11-12} paragraphs 47-49.c.
1516) AC Jonathan Swift’s conclusions in respect of the planning and recording of Brigade Control training in July 2019 {LFB00084097/3}.
1517) Brown {Day206/56:19-21}; {Day206/58:2-7}.
1518) George {LFB00032823/2}; Performance Information Folder: Operations, Prevention and Response for Performance CMB dated 12 February 2014 {LFB00042326/73}.
1519) Brown {Day206/53:5-17}.
1520) Brown {Day206/43:25}-{Day206/44:10}; {Day206/53:8-17}; Brown {LFB00032166/3} page 3, paragraph 5.
1521) Hayward {Day199/14:3-9}; {Day199/19:2-5}.
1522) Brown {Day206/44:4-10}; {Day206/52:12-17}.
1523) Brown {Day206/60:12-20}.
1524) Brown {Day206/49:21-25}.
1525) Hayward {Day199/37:16}-{Day199/38:8}.
1526) Hayward {Day199/37:19}-{Day199/38:8}; {Day199/95:17-20}; {Day199/100:21-25}; Brown {Day206/56:8-15}.
1527) Brown {LFB00032166/21} page 21, paragraph 66.
1528) Lakanal Control Report dated November 2012 {HOM00001124/49-50}.
1529) Brown {Day207/78:2-6}; {Day207/80:2-14}; Hayward {Day200/188:7-23}; {Day200/193:4}-{Day200/194:2}; {Day200/196:4-6}; {Day200/208:2-7}; {Day200/209:10-15}; Hayward {LFB00055191/24-25} pages 24-25, paragraphs 69-70; Emails between POM Hayward and SOM Bagnelle on 7-8 February 2013 {LFB00055221/1-3}.
1530) Brown {LFB00084020/12-13} pages 12-13, paragraph 28; Brown {Day206/50:19}-{Day206/52:5}.
1531) Brown {Day206/50:19}-{Day206/52:5}; Hayward {Day199/18:20}-{Day199/19:17}.
1532) Phase 1 Report Volume IV {INQ00014817/133} paragraph 28.130.
1533) Phase 1 Report Volume IV {INQ00014817/133} paragraph 28.131.
1534) Christopher Johnson {Day189/8:14}.
1535) Christopher Johnson {Day189/45:1-11}; {Day189/45:12-25}; Policy 700 {LFB00001762}.
1536) {LFB00000736}: this policy was extant at the time of the Grenfell Tower fire. The Inquiry does not have a copy of the policy in place at the time of the Lakanal House fire.
1537) As summarised in Ellis {LFB00089131/7-9} pages 7-9, paragraph 26.
1538) Radio repeaters are explained further below but, in summary, they are items of equipment intended to extend the range of a radio signal.
1539) Christopher Johnson {Day189/9:22}-{Day189/10:1-3}.
1540) Johnson, Communications Expert Report {CWJ00000119/142} paragraph 6.6.5; Christopher Johnson {Day189/16:1}-{Day189/17:12}.
1541) Christopher Johnson {Day189/25:14}-{Day189/26:16}.
1542) Johnson, Communications Expert Report {CWJ00000119/42} paragraph 3.2.5 - 3.2.13; Christopher Johnson {Day189/26:17}-{Day189/29:4}.
1543) Reason {Day182/39:18}-{Day182/40:13}; {Day181/204:12}-{Day181/205:9}.
1544) Policy No. 458 {LFB00013039/2} fourth bullet point. The general prohibition may be lifted where BARIE radios are unavailable and, following a risk assessment, the incident commander consents to the use of UHF radios.
1545) Christopher Johnson {Day189/44:4-20}; Ellis {LFB00089131/7} page 7, paragraph 21.
1546) Johnson, Communications Expert Report {CWJ00000119/55} paragraph 4.2.7.
1547) Christopher Johnson {Day189/38:5}-{Day189/39:9}.
1548) Johnson, Communications Expert Report {CWJ00000119/151} paragraph 6.9.4.
1549) Johnson, Communications Expert Report {CWJ00000119/43} paragraphs 3.2.15 - 3.2.16; Christopher Johnson {Day189/14:1}-{Day189/15:10}.
1550) Christopher Johnson {Day189/21:5}-{Day189/22:2}.
1551) Christopher Johnson {Day189/97:1}-{Day189/98:7}; {Day189/100:2-21}.
1552) Christopher Johnson {Day189/100:2-21}.
1553) Christopher Johnson {Day189/103:4}-{Day189/104:5}; {Day189/107:10-14}.
1554) Christopher Johnson {Day189/97:1}-{Day189/98:7}.
1555) Christopher Johnson {Day189/99:6-20}.
1556) Johnson, Communications Expert Report {CWJ00000119/181} paragraph 7.4.2.
1557) Christopher Johnson {Day189/11:3-20}.
1558) In the way that channel 3 was used to relay fire survival guidance information on the night of the fire: Johnson, Communications Expert Report {CWJ00000119/149} paragraph 6.8.9.
1559) Johnson, Communications Expert Report {CWJ00000119/176} paragraph 7.2.4; Christopher Johnson {Day189/51:12}-{Day189/52:19}; Dobson {Day212/45:23}-{Day212/46:4}.
1560) Christopher Johnson {Day189/136:1-12}.
1561) Dobson {Day212/45:1}-{Day212/46:11}; Reason {Day182/24:16-22}; {Day182/50:3-14}.
1562) Christopher Johnson {Day189/54:14-25}.
1563) Lakanal House Inquest – Day 42 Transcript {CWJ00000010/73-74}.
1564) Johnson, Communications Expert Report {CWJ00000119/193}.
1565) Training packages on communications were developed following the Lakanal House fire as part of TCAP 0039, but were not released before the Grenfell Tower fire. In any event, those packages gave only a description of the operation and set up of repeaters and leaky feeders and did not distinguish between the two {LFB00122846}; {LFB00122844}.
1566) Ashman {LFB00102269/3} page 3, paragraphs 11-12.
1567) Christopher Johnson {Day189/8:9-23}.
1568) {LFB00084685/25} paragraph 85; Reason {Day182/87:7-15}.
1569) Christopher Johnson {Day189/177:18-23}; {LFB00033375/2}.
1570) Christopher Johnson {Day189/57:11-23}; Christopher Johnson {Day189/58:9-12}.
1571) Christopher Johnson {Day189/58:14}-{Day189/59:4}.
1572) Christopher Johnson {Day189/59:5-10}.
1573) Christopher Johnson {Day189/59:11}-{Day189/60:9}.
1574) Christopher Johnson {Day189/93:20}-{Day189/94:12}.
1575) {LFB00089144/2} paragraph 3.1.
1576) Christopher Johnson {Day189/159:11-20}; {LFB00012913/10} section 13.
1577) Christopher Johnson {Day189/181:5-24}.
1578) Dobson {Day212/8:24}-{Day212/9:4}.
1579) Johnson, Communications Expert Report {CWJ00000119/59-60}; Johnson, Communications Expert Report {CWJ00000119/183}.
1580) Johnson, Communications Expert Report {CWJ00000119/60-61}.
1581) Johnson, Communications Expert Report {CWJ00000119/183-185}.
1582) Incident Communications Final Report {CWJ00000092}.
1583) Johnson, Communications Expert Report {CWJ00000119/64-66}; Dobson {Day212/9:21}-{Day212/11:24}.
1584) London Assembly’s Report of the 7th July Review Committee {CWJ00000007/22} paragraph 2.30; cited in Johnson, Communications Expert Report {CWJ00000119/70-71} paragraph 4.9.12.
1585) Johnson, Communications Expert Report {CWJ00000119/68-71}; Johnson, Communications Expert Report {CWJ00000119/185-187}.
1586) {LFB00001843/61} paragraph 9.3.11; Dobson {LFB00110652/3} page 3, paragraph 11; {LFB00041759}; {LFB00110654}; {LFB00001256/3} paragraph 2.9.
1587) {LFB00001255/9}.
1588) {LFB00029438/55} paragraph 6B3.24.
1589) An entry control officer manages the deployment of firefighters wearing breathing apparatus. For more information, see the Phase 1 Report Volume I, paragraphs 7.70 - 7.71.
1590) Dobson {Day212/12:24}-{Day212/13:10}.
1591) Reason {Day182/6:21-25}.
1592) {LFB00110657}.
1593) {LFB00110659}.
1594) Reason {Day182/3:15-23}; {Day182/4:18}-{Day182/5-22}.
1595) {LFB00034805/59}.
1596) {LFB00098635}; {LFB00098636}; Reason {Day181/208:8-11}.
1597) Reason {Day181/207:20}-{Day181/208:20}; {Day182/41:7-10}.
1598) {LFB00031268}.
1599) {LFB00031268/83-84}.
1600) Dobson {Day212/40:2}-{Day212/41:14}.
1601) Dobson {Day212/13:17}-{Day212/15:7}.
1602) Dobson {Day212/47:16-21}.
1603) {LFB00106755}.
1604) Reason {Day182/15:3-14}.
1605) {LFB00032158/3}.
1606) {LFB00042089}.
1607) {LFB00042089/8}.
1608) For a more detailed explanation of this process and the equipment involved, see the Phase 1 Report Volume I, paragraphs 7.70 - 7.71.
1609) Reason {Day181/166:7}-{Day181/167:9}.
1610) {LFB00034062/9}.
1611) {LFB00098636}.
1612) {LFB00098635}; Reason {Day181/208:8-11}.
1613) {LFB00105466/1}.
1614) Groves {Day177/191:22}-{Day177/198:1}.
1615) Reason {Day182/43:1-15}; {Day182/44:3-9}.
1616) Dobson {Day212/20:19}-{Day212/21:8}.
1617) {LFB00004729}.
1618) {LFB00004729/7}.
1619) Reason {Day182/58:8-15}.
1620) Reason {Day182/60:9}-{Day182/63:17}; Groves {Day178/3:2-13}; {Day178/4:13-17}.
1621) Reason {Day182/63:18}-{Day182/67:13}.
1622) Reason {Day182/83:5-21}; {Day182/88:9-11}; {Day182/92:15}-{Day182/93:7}.
1623) Reason {Day182/67:14}-{Day182/68:3}.
1624) Groves {Day177/174:15}-{Day177/176:7}.
1625) Groves {Day177/179:2}-{Day177/181:3}; {Day177/197:7}-{Day177/198:1}.
1626) {LFB00107130/53}.
1627) Reason {Day182/16:24}-{Day182/17:8}; {Day182/18:10}-{Day182/19:8}.
1628) Reason {Day182/19:10-18}.
1629) Reason {Day182/19:19}-{Day182/22:2}.
1630) {LFB00100307} item 23.
1631) Reason {Day182/100:9-25}.
1632) {LFB00088188} first row.
1633) {LFB00106755}.
1634) In his statement to the MPS, Dominic Ellis explained that the LFB’s working assumption was that the wattage of the other channels was based on previous radios held by the LFB, known as the Maxon radio. Director Reason’s evidence was that the Maxon radios were replaced by the HX series in 2007/2008, following the Bethnal Green fire in 2004: Reason {Day182/57:1-6}. There is no evidence, whether in this statement or elsewhere, that the issue of restricted wattage had been rectified by 14 June 2017: Ellis {MET00077839/9} page 9.
1635) Johnson, Communications Expert Report {CWJ00000119/48} paragraphs 3.5.8 and 3.5.9.
1636) {LFB00034062/10}.
1637) {LFB00042089/8}.
1638) Christopher Johnson {Day189/88:20}-{Day189/89:22}.
1639) Reason {Day181/179:18}-{Day181/180:7}.
1640) Christopher Johnson {Day189/80:13}-{Day189/81:4}.
1641) Johnson, Communications Expert Report {CWJ00000119/50} paragraphs 3.5.10 - 3.5.15.
1642) Reason {Day182/40:22-25}-{Day182/41:1-10}; Christopher Johnson {Day189/32:12}-{Day189/33:21}.
1643) Johnson, Communications Expert Report {CWJ00000119/159} paragraph 6.14.1.
1644) Christopher Johnson {Day189/108:5-9}; {Day189/115:1}-{Day189/122:3}.
1645) This was acknowledged by the LFB in its testing methodology {LFB00084087/3}.
1646) Johnson, Communications Expert Report {CWJ00000119/43} paragraphs 3.2.15 – 3.2.18; Christopher Johnson {Day189/15:11-18}.
1647) Groves {Day177/192:6}-{Day177/194:4}; Reason {Day182/60:9}-{Day182/63:17}; {Day182/63:18}-{Day182/67:14}.
1648) Phase 1 Report Volume IV {INQ00014817/133} paragraph 28.130.
1649) Although Commissioner Dobson thought that wholesale loss of communications was covered in training Dobson {Day212/49:18}-{Day212/50:6}, it was clear from Mr Groves’ evidence that that was not the case: Groves {Day177/192:6}-{Day177/194:4}.
1650) Christopher Johnson {Day189/198:3}-{Day189/199:6}.
1651) Christopher Johnson {Day189/202:2}-{Day189/208:1}.
1652) Christopher Johnson {Day189/95:2}-{Day189/96:2}.
1653) Section 38 of the Fire and Rescue Services Act 2004.
1654) Section 40 of the Fire and Rescue Services Act 2004.
1655) Stoianov, Water Expert Report {ISTRP00000008/229} paragraphs 3-5.
1656) Stoianov, Water Expert Report {ISTRP00000008/237}.
1657) Regulation 17G(1) of the Water Supply and Sewerage Services (Customer Service Standards) Regulations 2008.
1658) Stoianov, Water Expert Report {ISTRP00000005/48} paragraph 2; Stoianov, Water Expert Report {ISTRP00000008/234-5} paragraph 29.
1659) Stoianov, Water Expert Report {ISTRP00000003/5}.
1660) Stoianov, Water Expert Report {ISTRP00000008/229}.
1661) Stoianov {Day288/12:4-12}; Stoianov, Water Expert Report {ISTRP00000003/8-9}.
1662) Stoianov, Water Expert Report {ISTRP00000003/17-18}.
1663) Stoianov, Water Expert Report {ISTRP00000003/20}.
1664) Stoianov {Day288/19:3-9}.
1665) Stoianov, Water Expert Report {ISTRP00000006/3}; Stoianov {Day288/23:17}-{Day288/24:18}.
1666) Stoianov, Water Expert Report {ISTRP00000008/76}.
1667) Stoianov, Water Expert Report {ISTRP00000008/78}.
1668) Stoianov, Water Expert Report {ISTRP00000008/86}.
1669) Stoianov, Water Expert Report {ISTRP00000008/79}.
1670) Stoianov, Water Expert Report {ISTRP00000006/8}.
1671) Stoianov {Day288/30:16-19}.
1672) Stoianov, Water Expert Report {ISTRP00000006/7} ‘Jet B’.
1673) Stoianov, Water Expert Report {ISTRP00000006/7} ‘Jet D’.
1674) Stoianov, Water Expert Report {ISTRP00000006/7} ‘Jet E’.
1675) Stoianov {Day288/31:3-10}.
1676) Stoianov, Water Expert Report {ISTRP00000006/7} ‘Jet C’.
1677) Stoianov, Water Expert Report {ISTRP00000006/8}; {ISTRP00000006/26} ‘Jet H’.
1678) Stoianov {Day288/28:14-16}.
1679) Stoianov, Water Expert Report {ISTRP00000006/7-8} ‘Jet A’, ‘Jet H’, ‘Jet I’, ‘Jet J’.
1680) Stoianov, Water Expert Report {ISTRP00000006/7-8}; {ISTRP00000006/25-26} Jet F’, ‘Jet G’, ‘Jet I’, ‘Jet J’.
1681) Stoianov, Water Expert Report {ISTRP00000006/18}.
1682) Stoianov, Water Expert Report {ISTRP00000006/8} ‘Supply K’.
1683) Stoianov, Water Expert Report {ISTRP00000006/236} paragraph 2.
1684) Stoianov, Water Expert Report {ISTRP00000006/236} paragraph 2.
1685) Stoianov, Water Expert Report {ISTRP00000006/20} lines 31-32.
1686) Stoianov, Water Expert Report {ISTRP00000006/24} lines 8-9.
1687) Stoianov, Water Expert Report {ISTRP00000006/174} lines 26-28.
1688) Stoianov, Water Expert Report {ISTRP00000006/238} paragraph 3; Stoianov {Day288/42:12}-{Day288/43:23}.
1689) Stoianov {Day288/62:1}-{Day288/63:3}.
1690) {LFB00123672}, ‘Flow tests conducted on aerial appliance types used at Grenfell Tower fire’.
1691) {LFB00123672/16}, ‘Conclusions’’ {ISTRP00000006/236-238}.
1692) Stoianov, Water Expert Supplemental Report {ISTRPS00000001/21-28}.
1693) Stoianov {Day288/53:4}-{Day288/56:20}.
1694) Stoianov {Day288/57:7-19}.
1695) Stoianov {Day288/58:8}-{Day288/59:4}.
1696) Stoianov {Day288/59:6-14}.
1697) Stoianov {Day288/59:6-14}.
1698) Stoianov {Day288/59:15-25}.
1699) Stoianov, Water Expert Report {ISTRP00000006/20} lines 20-28.
1700) Stoianov, Water Expert Report {ISTRP00000006/23} lines 17-24.
1701) Stoianov, Water Expert Report {ISTRP00000006/22} lines 24-29; {ISTRP00000006/24} line 30 -{ISTRP00000006/25} line 2.
1702) Stoianov, Water Expert Report {ISTRP00000006/23} lines 25-30.
1703) Stoianov {Day288/64:22}-{Day288/65:7}.
1704) Stoianov, Water Expert Report {ISTRP00000006/24-25}.
1705) Stoianov, Water Expert Report {ISTRP00000006/238} paragraph 6; Stoianov {Day288/91:14-19}.
1706) Stoianov, Water Expert Report {ISTRP00000006/11}lines 32-37; {ISTRP00000006/239} paragraph d.
1707) Stoianov {Day288/91:14-19}.
1708) Stoianov, Water Expert Report {ISTRP00000006/238} paragraph 6; Stoianov {Day288/91:7-11}.
1709) Section 57 of the Water Industry Act 1991.
1710) “Specification for underground fire hydrants and surface box frames and covers”.
1711) {BSI00001767/13} paragraph 10.2.
1712) Stoianov {Day288/69:20-24}.
1713) Stoianov, Water Expert Report {ISTRP00000008/100}; Dr Stoianov also tested three other hydrants in the vicinity of Grenfell Tower. All three had similar flow coefficients of between 32 and 58.
1714) Stoianov {Day288/77:9}-{Day288/78:5}.
1715) Stoianov, Water Expert Report {ISTRP00000008/100}.
1716) Section 42 of the Fire and Rescue Services Act 2004.
1717) Stoianov, Water Expert Report {ISTRP00000009/21} paragraph 2.
1718) See {THA00000036}.
1719) Stoianov {Day288/85:8}-{Day288/86:13}.
1720) Stoianov {Day288/87:16-21}.
1721) Stoianov, Water Expert Report {ISTRP00000008/79} lines 24-26; {ISTRP00000008/81} figure 6-37.
1722) {THA00000012/2}.
1723) Stoianov, Water Expert Report {ISTRP00000009/91-92}.
1724) Stoianov, Water Expert Report {ISTRP00000009/85} paragraph 1(a).
1725) Stoianov, Water Expert Report {ISTRP00000009/85} paragraph 1(b).
1726) Stoianov, Water Expert Report {ISTRP00000009/26} lines 12-17; Stoianov {Day288/94:16}-{Day 288/95:1}.
1727) Stoianov, Water Expert Report {ISTRP00000009/85} paragraph 2; Stoianov, Water Expert Report {ISTRP00000008/213-214}.
1728) Stoianov {Day288/95:24}-{Day288/96:8}.
1729) Stoianov, Water Expert Report {ISTRP00000009/86} paragraph 4.
1730) Stoianov, Water Expert Report {ISTRP00000005/8} section 4.1.2.1.
1731) Stoianov, Water Expert Report {ISTRP00000008/47-48}; {ISTRP00000008/224} lines 9-13.
1732) Stoianov, Water Expert Report {ISTRP00000008/231} paragraph 13.
1733) Stoianov, Water Expert Report {ISTRP00000009/103-104} paragraph 52.
1734) Stoianov {Day288/111:12-20}.
1735) Stoianov, Water Expert Report {ISTRP00000009/106} section 7.8.7.
1736) Stoianov, Water Expert Report {ISTRP00000008/236} paragraph (iii); Stoianov {Day288/107:6-21}.
1737) Stoianov, Water Expert Report {ISTRP00000008/11} paragraph 1.
1738) Stoianov, Water Expert Report {ISTRP00000009/30}.
1739) Stoianov, Water Expert Report {ISTRP00000009/102-103}; {ISTRP00000009/106} paragraph 59.
1740) Stoianov {Day288/104:12}-{Day288/105:14}.
1741) Stoianov, Water Expert Report {ISTRP00000009/99-102}.
1742) Stoianov, Water Expert Report {ISTRP00000009/97} paragraph b; Stoianov, {ISTRP00000009/91} paragraph 19(a).
1743) Stoianov, Water Expert Report {ISTRP00000006/239-240} paragraph 8(a); Stoianov, Water Expert Report {ISTRP00000009/89} paragraph (b).
1744) Stoianov, Water Expert Report {ISTRP00000009/98} paragraph (e); see also {ISTRP00000009/101} paragraph (c).
1745) Phase 1 Report Volume IV paragraph 28.132.
1746) Phase 1 Report Volume IV paragraph 28.133.
1747) McGuirk, Firefighting Expert Report {SMC00000046/68-69} paragraph 183.
1748) Stoianov, Water Expert Report {ISTRP00000006/7-8}.
1749) Policy 822: Operational use of aerial appliances {LFB00000189}.
1750) McGuirk, Firefighting Expert Report {SMC00000046/64} paragraph 170.
1751) Stoianov, Water Expert Report {ISTRP00000006/24} lines 8-9.
1752) McGuirk, Firefighting Expert Report {SMC00000046/64} paragraph 170.
1753) Stoianov, Water Expert Report {ISTRP00000006/238} lines 20-22.
1754) Stoianov, Water Expert Report {ISTRP00000006/67} lines 14-16; {ISTRP00000006/69}.
1755) Stoianov, Water Expert Report {ISTRP00000006/65}; {ISTRP00000008/73} lines 18-24; {LFB00024354}.
1756) Stoianov, Water Expert Report {ISTRP00000009/4}; {ISTRP00000009/7}.
1757) Stoianov, Water Expert Report {ISTRP00000009/93}.
1758) Phase 1 hearings: {Day34/84:9-19}; Stoianov, Water Expert Report {ISTRP00000009/93}.
1759) McGuirk, Firefighting Expert Report {SMC00000046/73} paragraphs 199-201.
1760) Phase 1 Report Volume III paragraph 16.87; Wilson {MET00019953/3-4}, pages 3-4.
1761) McGuirk, Firefighting Expert Report {SMC00000046/73} paragraphs 199-201; McGuirk {Day190/140:3-5}.
1762) McGuirk, Firefighting Expert Report {SMC00000046/73} paragraph 201.
1763) McGuirk {Day190/140:11}-{Day190/141:10}.
1764) McGuirk, Firefighting Expert Report {SMC00000046/76} paragraph 207; ORR v0.7 {LFB00032988/501}.
1765) McGuirk, Firefighting Expert Report {SMC00000046/76} paragraph 207.
1766) McGuirk {Day190/157:144}-{Day190/158:11}.
1767) McGuirk {Day190/158:13}-{Day190/159:7}.
1768) Phase 1 Report Volume II paragraphs 12.3-12.5, 13.18-13.19, 13.69-13.70 and 14.112-14.114.
1769) Grimwood {Day188/54:12}-{Day188/55:16}.
1770) McGuirk, Firefighting Expert Report {SMC00000046/85} paragraph 235; McGuirk {Day190/163:9-16}.
1771) Phase 1 Report Volume IV paragraph 28.1.
1772) “Effectiveness, efficiency and people 2018/19 – London Fire Brigade” pages 30-33.